

Clinical and microbiological efficacy of continuous versus intermittent application of meropenem in critically ill patients: a randomized open-label controlled trial
- PMID: 22742765
- PMCID: PMC3580671
- DOI: 10.1186/cc11405
Clinical and microbiological efficacy of continuous versus intermittent application of meropenem in critically ill patients: a randomized open-label controlled trial
Abstract
Introduction: Meropenem bactericidal activity depends on the time when the free drug concentrations remain above the minimum inhibitory concentration of pathogens. The goal of this study was to compare clinical and bacteriological efficacy of continuous meropenem infusion versus bolus administration in critically ill patients with severe infection, and to evaluate the safety of both dosing regimens.
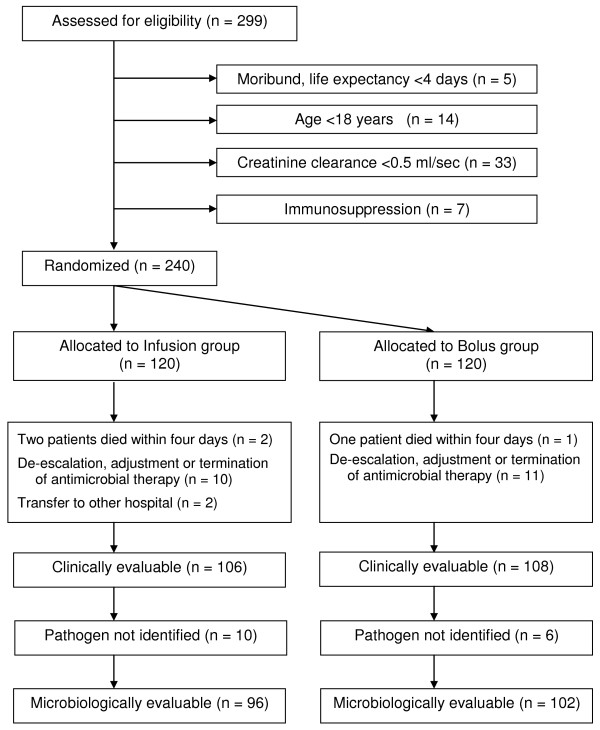
Methods: Patients admitted to the interdisciplinary Intensive Care Unit (ICU) who suffered from severe infections and received meropenem were randomized either in the Infusion group (n = 120) or in the Bolus group (n = 120). Patients in the Infusion group received a loading dose of 2 g of meropenem followed by a continuous infusion of 4 g of meropenem over 24 hours. Patients in the Bolus group were given 2 g of meropenem over 30 minutes every 8 hours. Clinical and microbiological outcome, safety, meropenem-related length of ICU and hospital stay, meropenem-related length of mechanical ventilation, duration of meropenem treatment, total dose of meropenem, and ICU and in-hospital mortality were assessed.
Results: Clinical cure at the end of meropenem therapy was comparable between both groups (83.0% patients in the Infusion vs. 75.0% patients in the Bolus group; P = 0.180). Microbiological success rate was higher in the Infusion group as opposed to the Bolus group (90.6% vs. 78.4%; P = 0.020). Multivariate logistic regression identified continuous administration of meropenem as an independent predictor of microbiological success (OR = 2.977; 95% CI = 1.050 to 8.443; P = 0.040). Meropenem-related ICU stay was shorter in the Infusion group compared to the Bolus group (10 (7 to 14) days vs. 12 (7 to 19) days; P = 0.044) as well as shorter duration of meropenem therapy (7 (6 to 8) days vs. 8 (7 to 10) days; P = 0.035) and lower total dose of meropenem (24 (21 to 32) grams vs. 48 (42 to 60) grams; P < 0.0001). No severe adverse events related to meropenem administration in either group were observed.
Conclusions: Continuous infusion of meropenem is safe and, in comparison with higher intermittent dosage, provides equal clinical outcome, generates superior bacteriological efficacy and offers encouraging alternative of antimicrobial therapy in critically ill patients.
Figures
Comment in
-
Continuous infusion of meropenem in critically ill patients: practical considerations.Crit Care. 2012 Aug 27;16(4):444. doi: 10.1186/cc11459. Crit Care. 2012. PMID: 22958536 Free PMC article. No abstract available.
Similar articles
-
Evaluation of Meropenem Extended Versus Intermittent Infusion Dosing Protocol in Critically Ill Patients.J Intensive Care Med. 2020 Aug;35(8):763-771. doi: 10.1177/0885066618784264. Epub 2018 Jun 28. J Intensive Care Med. 2020. PMID: 29954243
-
Pharmacokinetic and Pharmacodynamic Efficacies of Continuous versus Intermittent Administration of Meropenem in Patients with Severe Sepsis and Septic Shock: A Prospective Randomized Pilot Study.Chin Med J (Engl). 2017 May 20;130(10):1139-1145. doi: 10.4103/0366-6999.205859. Chin Med J (Engl). 2017. PMID: 28485312 Free PMC article. Clinical Trial.
-
[Comparison of 3-hour and 30-minute infusion regimens for meropenem in patients with hospital acquired pneumonia in intensive care unit: a randomized controlled clinical trial].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2014 Sep;26(9):644-9. doi: 10.3760/cma.j.issn.2095-4352.2014.09.008. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2014. PMID: 25230866 Clinical Trial. Chinese.
-
Evaluation of studies on extended versus standard infusion of beta-lactam antibiotics.Am J Health Syst Pharm. 2019 Sep 3;76(18):1383-1394. doi: 10.1093/ajhp/zxz154. Am J Health Syst Pharm. 2019. PMID: 31505562 Review.
-
Clinical outcomes of prolonged infusion (extended infusion or continuous infusion) versus intermittent bolus of meropenem in severe infection: A meta-analysis.PLoS One. 2018 Jul 30;13(7):e0201667. doi: 10.1371/journal.pone.0201667. eCollection 2018. PLoS One. 2018. PMID: 30059536 Free PMC article. Review.
Cited by
-
Continuous infusion of piperacillin/tazobactam in septic critically ill patients--a multicenter propensity matched analysis.PLoS One. 2012;7(11):e49845. doi: 10.1371/journal.pone.0049845. Epub 2012 Nov 21. PLoS One. 2012. PMID: 23185458 Free PMC article.
-
Clinical outcomes of extended versus intermittent administration of piperacillin/tazobactam for the treatment of hospital-acquired pneumonia: a randomized controlled trial.Eur J Clin Microbiol Infect Dis. 2017 Mar;36(3):459-466. doi: 10.1007/s10096-016-2819-1. Epub 2016 Oct 28. Eur J Clin Microbiol Infect Dis. 2017. PMID: 27796647 Free PMC article. Clinical Trial.
-
Update of Sepsis in the Intensive Care Unit.J Innate Immun. 2017;9(5):441-455. doi: 10.1159/000477419. Epub 2017 Jul 12. J Innate Immun. 2017. PMID: 28697503 Free PMC article. Review.
-
Continuous infusion of meropenem in critically ill patients: practical considerations.Crit Care. 2012 Aug 27;16(4):444. doi: 10.1186/cc11459. Crit Care. 2012. PMID: 22958536 Free PMC article. No abstract available.
-
Management of Pneumonia and Blood Stream Infections with New Antibiotic Adjuvant Entity (Ceftriaxone + Sulbactam + Disodium Edetate)- A Novel Way to Spare Carbapenems.J Clin Diagn Res. 2016 Dec;10(12):LC23-LC27. doi: 10.7860/JCDR/2016/20904.9014. Epub 2016 Dec 1. J Clin Diagn Res. 2016. PMID: 28208889 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
