

Validation of methods for oropharyngeal cancer HPV status determination in US cooperative group trials
- PMID: 22743284
- PMCID: PMC6362985
- DOI: 10.1097/PAS.0b013e318253a2d1
Validation of methods for oropharyngeal cancer HPV status determination in US cooperative group trials
Abstract
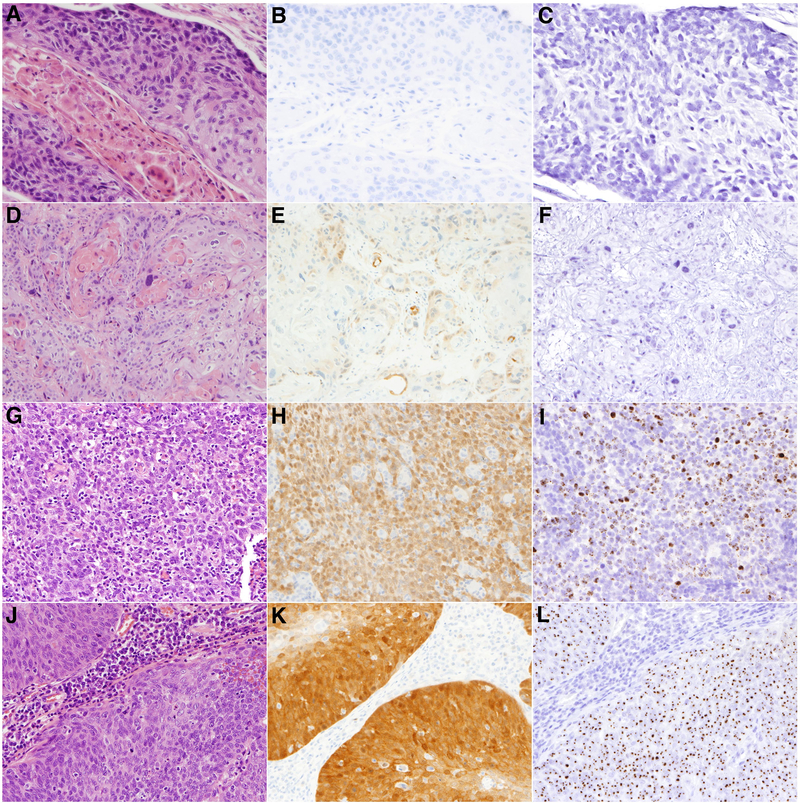
Tumor human papillomavirus (HPV) status is a prognostic factor for oropharyngeal cancer, but classification methods are not standardized. Here we validate the HPV classification methods used in US cooperative group trials. Tumor DNA and RNA purified from 240 paraffin-embedded oropharyngeal cancers diagnosed from 2000 to 2009 were scored as evaluable if positive for DNA and mRNA controls by quantitative polymerase chain reaction (PCR). Eighteen high-risk (HR) HPV types were detected in tumors by consensus PCR, followed by HR-HPV E6/7 oncogene expression analysis by quantitative reverse transcriptase PCR. The sensitivity (S), specificity (SP), and positive (PPV) and negative predictive values (NPV) of p16 expression detected by immunohistochemistry (IHC) and HPV16 detected by in situ hybridization (ISH) were evaluated in comparison with HR-HPV E6/7 oncogene expression. Interrater agreement among 3 pathologists was evaluated by κ statistics. Of 235 evaluable tumors, 158 (67%; 95% confidence interval, 61.2-73.3) were positive for HR-HPV E6/7 oncogene expression [HPV type 16 (92%), 18 (3%), 33 (3%), 35 (1%), or 58 (1%)]. p16 IHC had high sensitivity (S 96.8%, SP 83.8%, PPV 92.7%, and NPV 92.5%), whereas HPV16 ISH had high specificity (S 88.0%, SP 94.7%, PPV 97.2%, and NPV 78.9%) for HR-HPV oncogene expression. Interrater agreement was excellent for p16 (κ=0.95 to 0.98) and HPV16 ISH (κ=0.83 to 0.91). Receiver operating curve analysis determined the cross-product of p16 intensity score and percentage of tumor staining to optimally discriminate HR-HPV E6/7-positive and HR-HPV E6/7-negative tumors. p16 IHC and HPV16 ISH assays show excellent performance, with high sensitivity and specificity, respectively. A new validated H-score for p16 IHC assessment is proposed. Appropriate assay choice depends on clinical implications of a false-positive or false-negative test.
Conflict of interest statement
(Disclosures: Maura Gillison was the recipient of loaned equipment and reagents from Ventana Corp. that assisted with the study. The other authors have no conflicts of interest or funding to disclose)
Figures
References
-
- Ahmed A, Cascarini L, Sandison A, Clarke P. Survey of the use of tests for human papilloma virus and epidermal growth factor receptor for squamous cell carcinoma of the head and neck in UK head and neck multidisciplinary teams. Br J Oral Maxillofac Surg 2011; 3:1–5 - PubMed
-
- Begum S, Gillison ML, Ansari-Lari MA, Shah K, Westra WH. Detection of human papillomavirus in cervical lymph nodes: a highly effective strategy for localizing site of tumor origin. Clin Cancer Res 2003;9:6469–6475. - PubMed
-
- Begum S, Gillison ML, Nicol TL, Westra WH. Detection of human papillomavirus-16 in fine-needle aspirates to determine tumor origin in patients with metastatic squamous cell carcinoma of the head and neck. Clin Cancer Res 2007;13:1186–1191. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
