

Characterization of platelet dysfunction after trauma
- PMID: 22743367
- PMCID: PMC3387387
- DOI: 10.1097/TA.0b013e318256deab
Characterization of platelet dysfunction after trauma
Abstract
Background: The increased morbidity and mortality associated with coagulopathy and thrombocytopenia after trauma are well described. However, few studies have assessed platelet function after injury.
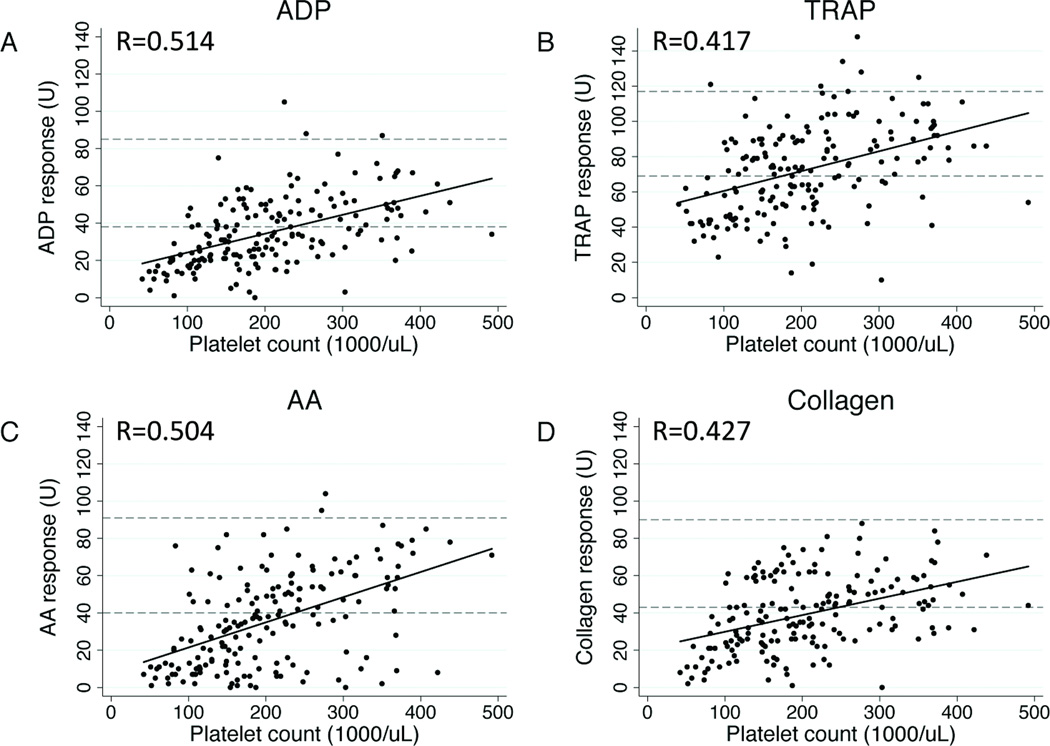
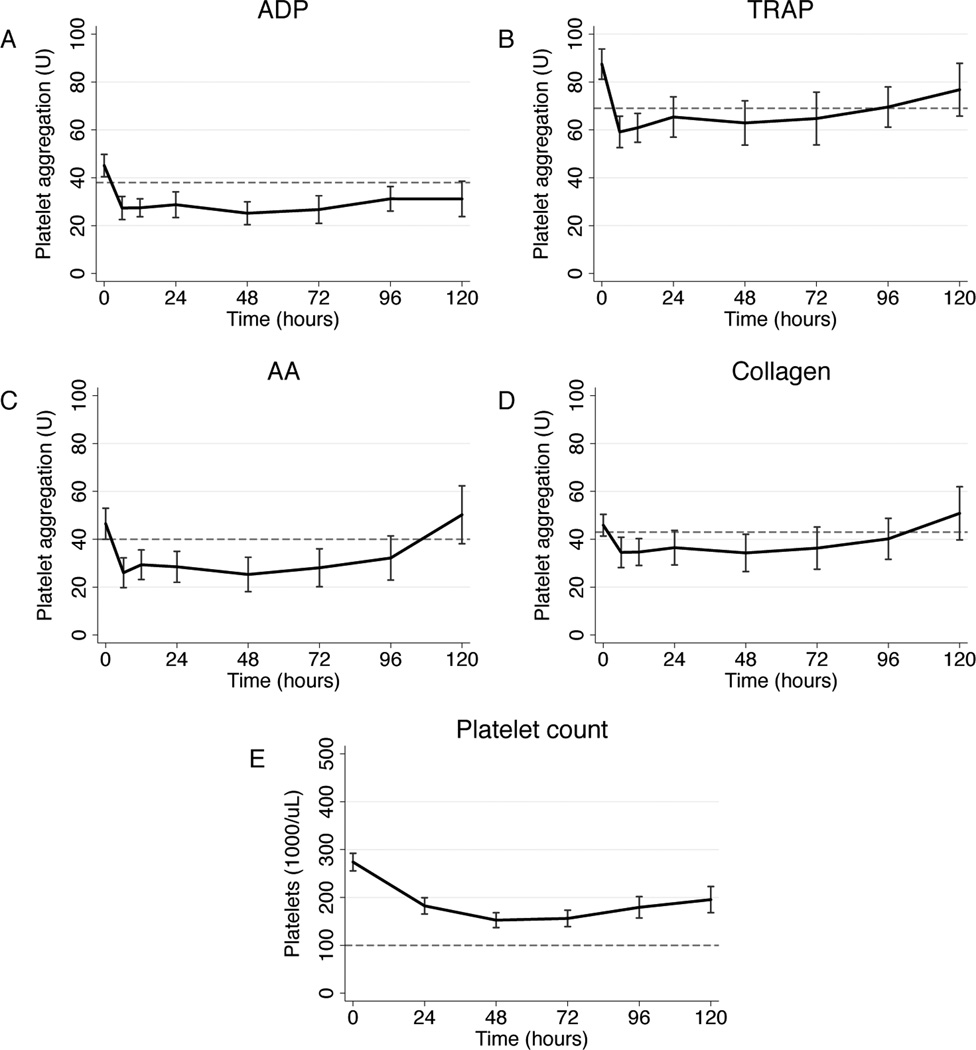
Methods: Blood samples were prospectively collected from 101 patients with critical injury and trauma on arrival to the emergency department and serially after admission to a Level I urban trauma intensive care unit from November 2010 to October 2011 and functionally assayed for responsiveness to adenosine diphosphate, thrombin receptor-activating peptide, arachidonic acid (AA), and collagen using multiple electrode impedance aggregometry.
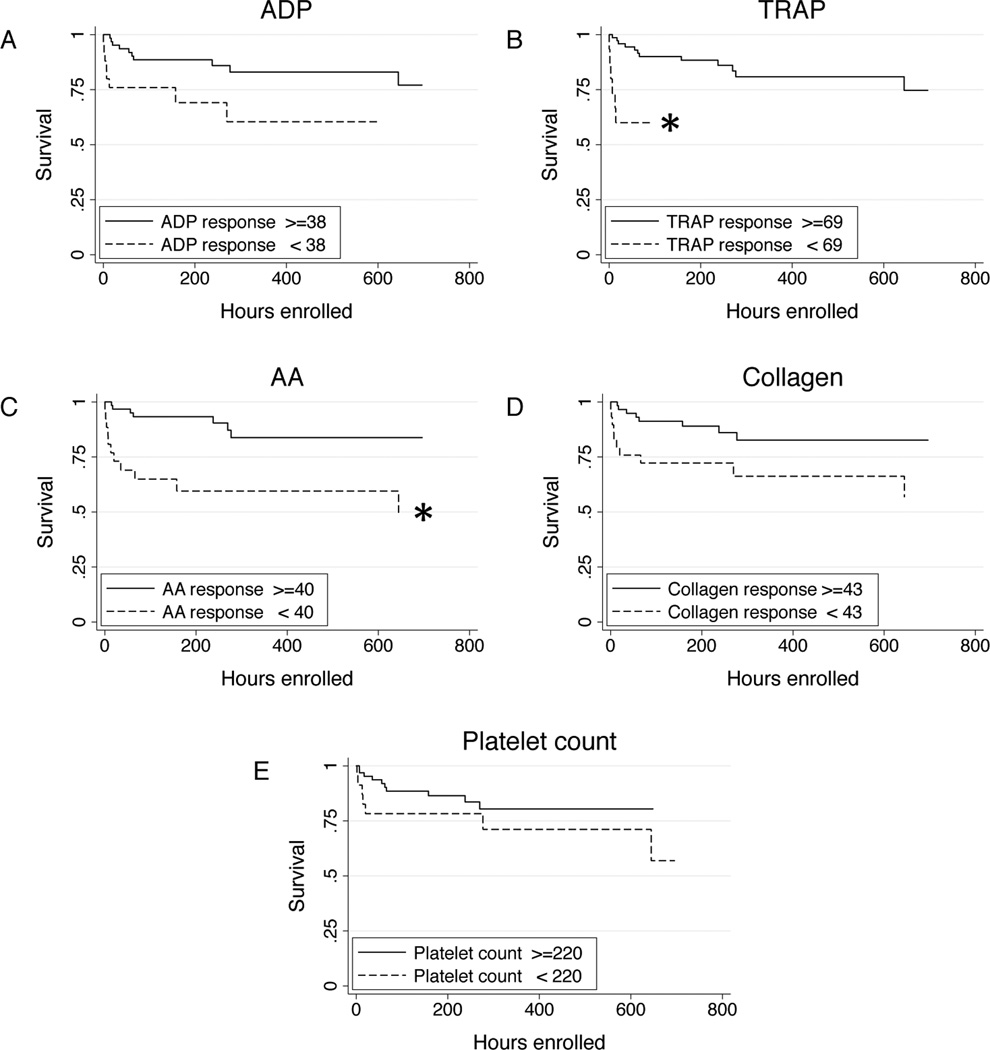
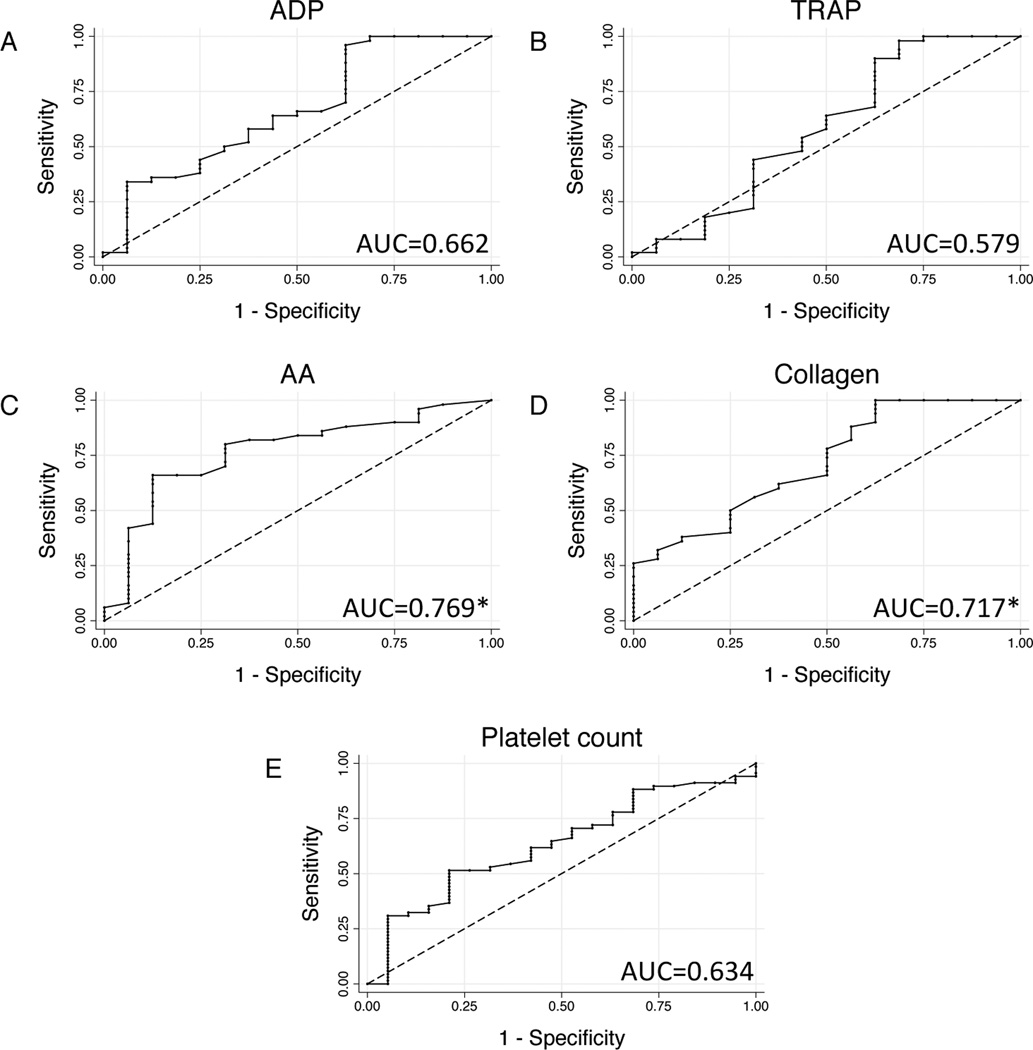
Results: Of the 101 enrolled patients, 46 (45.5%) had below-normal platelet response to at least one agonist ("platelet hypofunction") at admission, and 92 patients (91.1%) had platelet hypofunction some time during their intensive care unit stay. Admission platelet hypofunction was associated with low Glasgow Coma Scale score and a nearly 10-fold higher early mortality. Logistic regression identified admission Glasgow Coma Scale (odds ratio, 0.819; p = 0.008) and base deficit (odds ratio, 0.872; p = 0.033) as independent predictors of platelet hypofunction. Admission AA and collagen responsiveness were significantly lower for patients who died (p < 0.01), whereas admission platelet counts were similar (p = 0.278); Cox regression confirmed thrombin receptor-activating peptide, AA, and collagen responsiveness as independent predictors of in-hospital mortality (p < 0.05). Receiver operating characteristic analysis identified admission AA and collagen responsiveness as negative predictors of both 24-hour (AA area under the curve [AUC], 0.874; collagen AUC, 0.904) and in-hospital mortality (AA AUC, 0.769; collagen AUC, 0.717).
Conclusion: In this prognostic study, we identify clinically significant platelet dysfunction after trauma in the presence of an otherwise reassuring platelet count and standard clotting studies, with profound implications for mortality. Multiple electrode impedance aggregometry reliably identifies this dysfunction in injured patients, and admission AA and collagen responsiveness are sensitive and specific independent predictors of both early and late mortality.
Conflict of interest statement
Conflicts of interest: The Multiplate® device was loaned and reagents provided by the distributor (DiaPharma Group, Inc; West Chester, OH) for this investigator-initiated study. There are no direct financial relationships between the authors and manufacturer.
Figures
References
-
- Davenport RA, Brohi K. Coagulopathy in trauma patients: importance of thrombocyte function? Curr Opin Anaesthesiol. 2009;22(2):261–266. - PubMed
-
- Schnuriger B, Inaba K, Abdelsayed GA, et al. The impact of platelets on the progression of traumatic intracranial hemorrhage. J Trauma. 2010;68(4):881–885. - PubMed
-
- Hess JR, Brohi K, Dutton RP, et al. The coagulopathy of trauma: a review of mechanisms. J Trauma. 2008;65(4):748–754. - PubMed
-
- Toth O, Calatzis A, Penz S, et al. Multiple electrode aggregometry: a new device to measure platelet aggregation in whole blood. Thromb Haemost. 2006;96(6):781–788. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
