

Criteria for empiric treatment of hyperfibrinolysis after trauma
- PMID: 22743377
- PMCID: PMC3781292
- DOI: 10.1097/TA.0b013e3182598c70
Criteria for empiric treatment of hyperfibrinolysis after trauma
Abstract
Background: Recent studies identify a survival benefit from the administration of antifibrinolytic agents in patients with severe injury and trauma. However, identification of hyperfibrinolysis requires thromboelastography, which is not widely available. We hypothesized that analysis of patients with thromboelastography-diagnosed hyperfibrinolysis would identify clinical criteria for empiric antifibrinolytic treatment in the absence of thromboelastography.
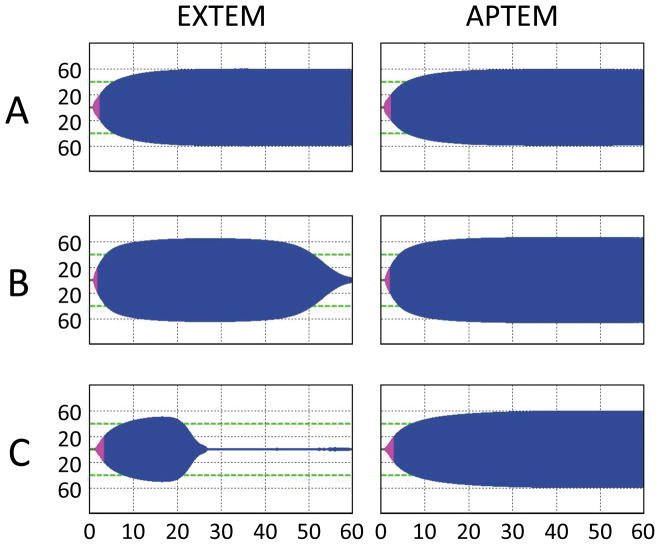
Methods: From November 2010 to March 2012, serial blood samples were collected from 115 patients with critical injury on arrival to the emergency department of an urban Level I trauma center. Rotational thromboelastography was performed to assess viscoelastic properties of clot formation in the presence and absence of aprotinin to identify treatable hyperfibrinolysis. For 20 patients identified with treatable hyperfibrinolysis, clinical predictors were investigated using receiver operating characteristic analysis.
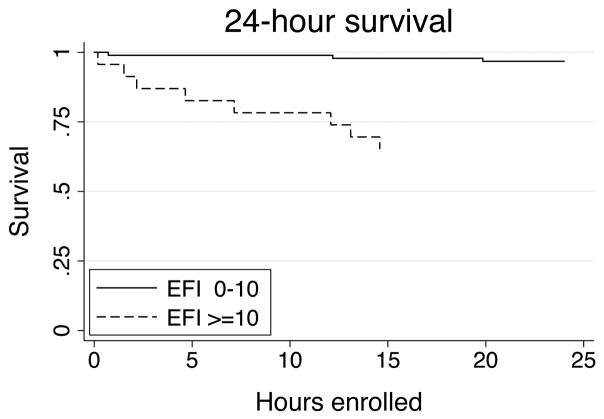
Results: Of the 115 patients evaluated, 20% had hyperfibrinolysis, defined as an admission maximal clot lysis of 10% or higher, reversible by aprotinin treatment. Patients with hyperfibrinolysis had significantly lower temperature, pH, and platelet counts and higher international normalized ratio, activated partial thromboplastin time, and D-dimer. Hyperfibrinolysis was associated with multiorgan failure (63.2% vs. 24.6%, p = 0.004) and mortality (52.2% vs. 12.9%, p < 0.001). We then evaluated all non-rotational thromboelastography clinical and laboratory parameters predictive of hyperfibrinolysis using receiver operating characteristic analysis to evaluate potential empiric treatment guidelines. The presence of hypothermia (temperature ≤36.0°C), acidosis (pH ≤7.2), relative coagulopathy (international normalized ratio ≥1.3 or activated partial thromboplastin time ≥30), or relative thrombocytopenia (platelet count ≤200) identified hyperfibrinolysis with 100% sensitivity and 55.4% specificity (area under the curve, 0.777).
Conclusion: Consideration of empiric antifibrinolytic therapy is warranted for patients with critical injury and trauma who present with acidosis, hypothermia, coagulopathy, or relative thrombocytopenia. These clinical predictors identified hyperfibrinolysis with 100% sensitivity while simultaneously eliminating 46.6% of inappropriate therapy compared with the empiric treatment of all injured patients. These criteria will facilitate empiric treatment of hyperfibrinolysis for clinicians without access to thromboelastography.
Level of evidence: Prognostic study, level III.
Conflict of interest statement
Conflicts of interest: The ROTEM® device was loaned and reagents provided by the distributor (Tem Innovations GmbH (formerly Pentapharm); Munich, Germany) for this investigator-initiated study. There are no direct financial relationships between the authors and manufacturer.
Figures
References
-
- Hess JR, Brohi K, Dutton RP, et al. The coagulopathy of trauma: a review of mechanisms. J Trauma. 2008;65(4):748–54. - PubMed
-
- Brohi K, Cohen MJ, Davenport RA. Acute coagulopathy of trauma: mechanism, identification and effect. Curr Opin Crit Care. 2007;13(6):680–5. - PubMed
-
- Holcomb JB, Wade CE, Michalek JE, et al. Increased plasma and platelet to red blood cell ratios improves outcome in 466 massively transfused civilian trauma patients. Ann Surg. 2008;248(3):447–58. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
