

Pathobiology of pulmonary arterial hypertension and right ventricular failure
- PMID: 22743666
- PMCID: PMC4019748
- DOI: 10.1183/09031936.00046612
Pathobiology of pulmonary arterial hypertension and right ventricular failure
Abstract
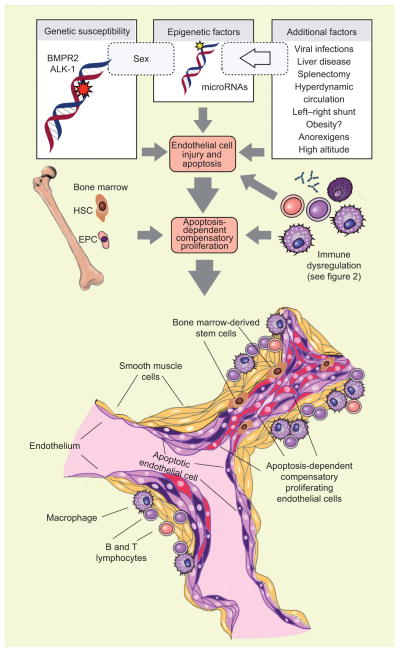
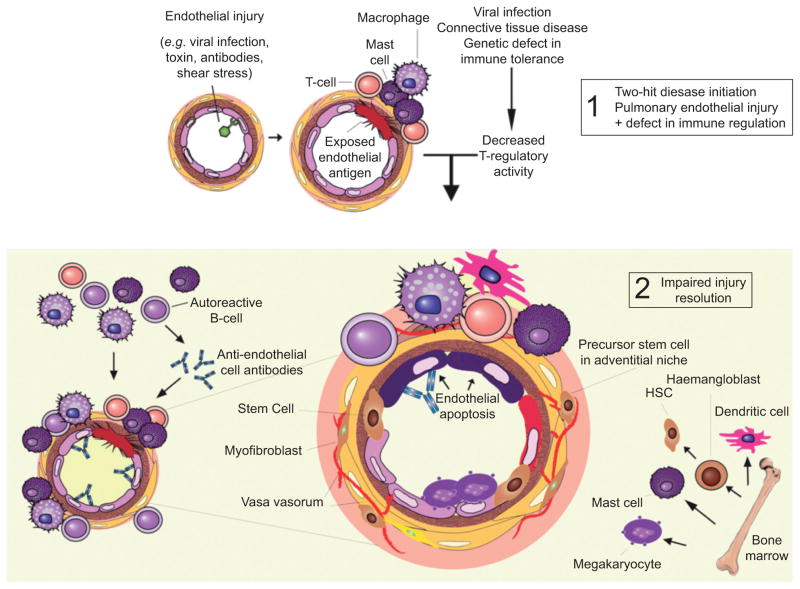
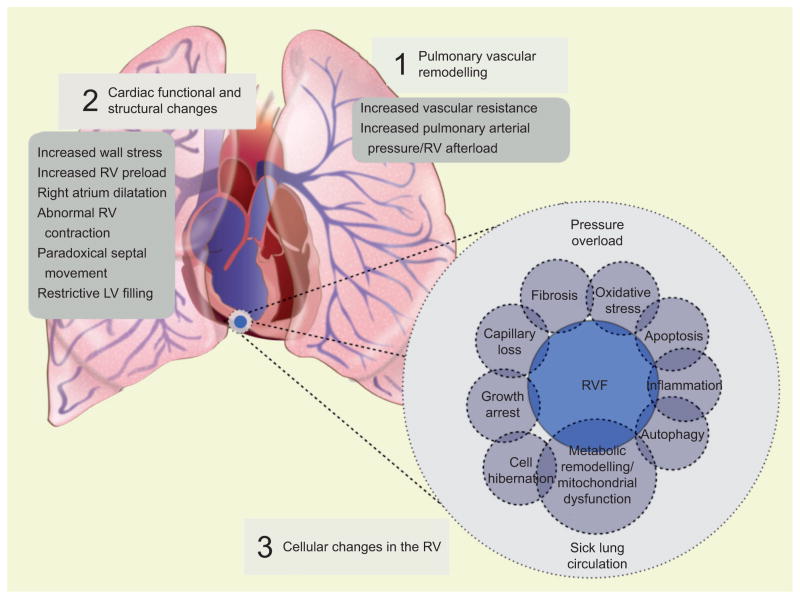
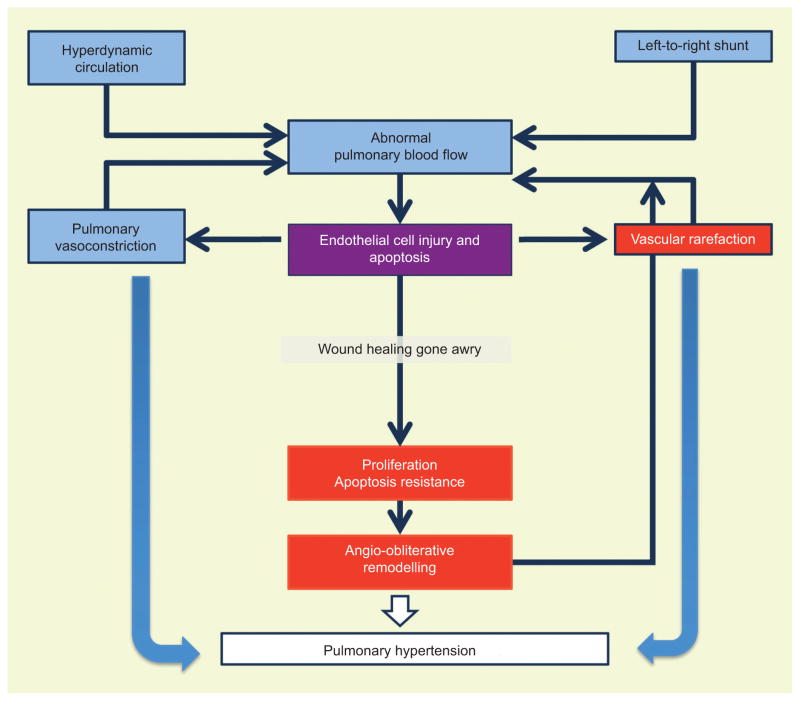
Pulmonary arterial hypertension (PAH) is no longer an orphan disease. There are three different classes of drugs for the treatment of PAH that are currently being used and an increasing number of patients are being treated with a single drug or combination therapy. During the last 25 yrs, new insights into the pathobiology of PAH have been gained. The classical mechanical concepts of pressure, flow, shear stress, right ventricle wall stress and impedance have been complemented with the new concepts of cell injury and repair and interactions of complex multicellular systems. Integrating these concepts will become critical as we design new medical therapies in order to change the prognosis of patients with these fatal diseases. This review intends to summarise recent pathobiological concepts of PAH and right ventricle failure mainly derived from human studies, which reflect the progress made in the understanding of this complex group of pulmonary vascular diseases.
Conflict of interest statement
None declared.
Figures
References
-
- Galie N, Hoeper M, Humbert M, et al. Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Respir J. 2009;34:1219–1263. - PubMed
-
- Frost AE, Badesch DB, Barst RJ, et al. The changing picture of patients with pulmonary arterial hypertension in the United States: how REVEAL differs from historic and non-US Contemporary Registries. Chest. 2011;139:128–137. - PubMed
-
- Humbert M, Sitbon O, Chaouat A, et al. Pulmonary arterial hypertension in France: results from a national registry. Am J Respir Crit Care Med. 2006;173:1023–1030. - PubMed
-
- Peacock AJ, Murphy NF, McMurray JJV, et al. An epidemiological study of pulmonary arterial hypertension. Eur Respir J. 2007;30:104–109. - PubMed
-
- Escribano-Subias P, Blanco I, López-Meseguer M, et al. Survival in pulmonary hypertension in Spain insights from the Spanish registry. Eur Respir J. 2012;40:596–603. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical