

Fluid overload and fluid removal in pediatric patients on extracorporeal membrane oxygenation requiring continuous renal replacement therapy
- PMID: 22743776
- PMCID: PMC3423554
- DOI: 10.1097/CCM.0b013e318258ff01
Fluid overload and fluid removal in pediatric patients on extracorporeal membrane oxygenation requiring continuous renal replacement therapy
Abstract
Objective: In pediatric patients, fluid overload at continuous renal replacement therapy initiation is associated with increased mortality. The aim of this study was to characterize the association between fluid overload at continuous renal replacement therapy initiation, fluid removal during continuous renal replacement therapy, the kinetics of fluid removal and mortality in a large pediatric population receiving continuous renal replacement therapy while on extracorporeal membrane oxygenation.
Design: Retrospective chart review.
Setting: Tertiary children's hospital.
Patients: Extracorporeal membrane oxygenation patients requiring continuous renal replacement therapy from July 2006 to September 2010.
Interventions: None.
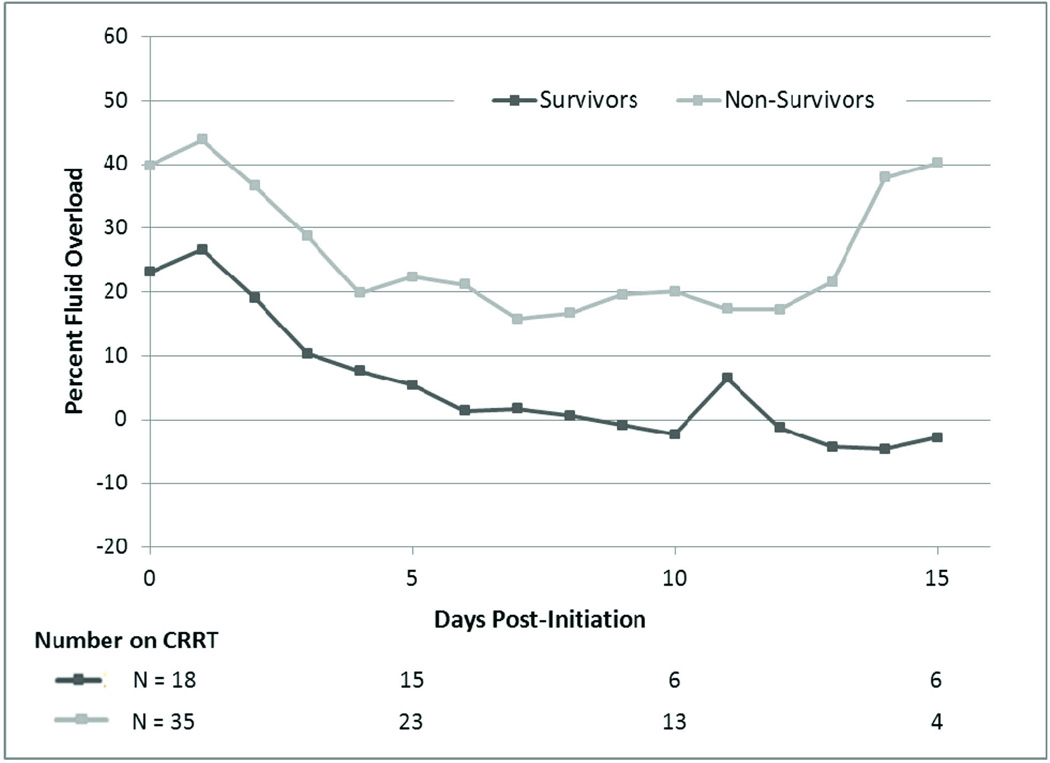
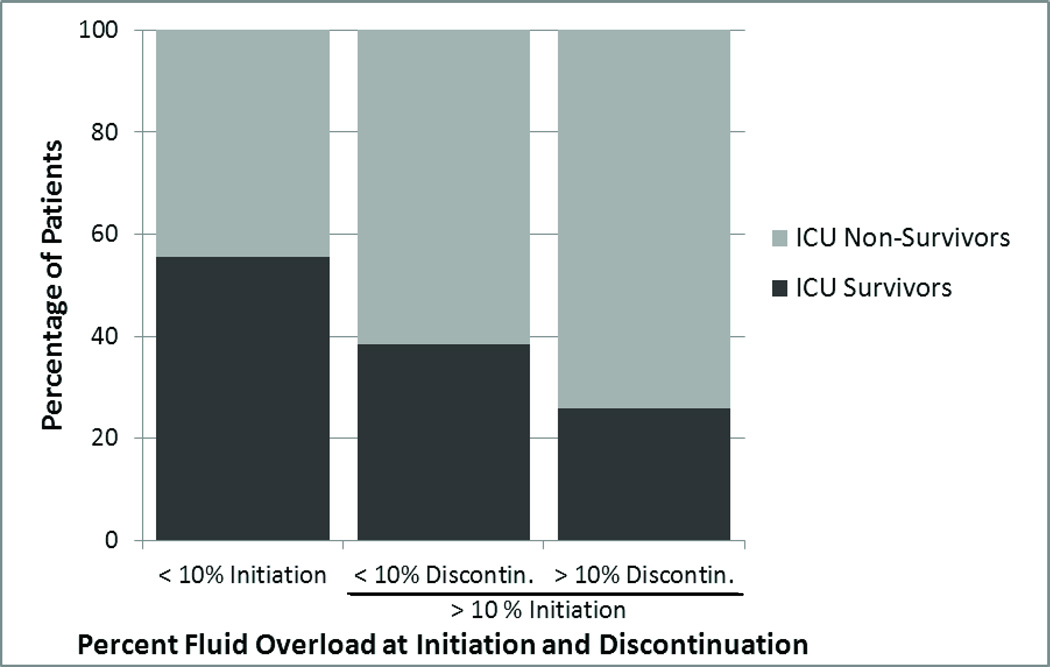
Measurements and main results: Overall intensive care unit survival was 34% for 53 patients that were initiated on continuous renal replacement therapy while on extracorporeal membrane oxygenation during the study period. Median fluid overload at continuous renal replacement therapy initiation was significantly lower in survivors compared to nonsurvivors (24.5% vs. 38%, p = .006). Median fluid overload at continuous renal replacement therapy discontinuation was significantly lower in survivors compared to nonsurvivors (7.1% vs. 17.5%, p = .035). After adjusting for percent fluid overload at continuous renal replacement therapy initiation, age, and severity of illness, the change in fluid overload at continuous renal replacement therapy discontinuation was not significantly associated with mortality (p = .212). Models investigating the rates of fluid removal in different periods, age, severity of illness, and fluid overload at continuous renal replacement therapy initiation found that fluid overload at continuous renal replacement therapy initiation was the most consistent predictor of survival.
Conclusions: Our data demonstrate an association between fluid overload at continuous renal replacement therapy initiation and mortality in pediatric patients receiving extracorporeal membrane oxygenation. The degree of fluid overload at continuous renal replacement therapy discontinuation is also associated with mortality, but appears to reflect the effect of fluid overload at initiation. Furthermore, correction of fluid overload to ≤ 10% was not associated with improved survival. These results suggest that intervening prior to the development of significant fluid overload may be more clinically effective than attempting fluid removal after significant fluid overload has developed. Our findings suggest a role for earlier initiation of continuous renal replacement therapy in this population, and warrant further clinical studies.
Conflict of interest statement
The authors have not disclosed any potential conflicts of interest.
Figures
Comment in
-
Lessons in advanced extracorporeal life support.Crit Care Med. 2012 Sep;40(9):2729-31. doi: 10.1097/CCM.0b013e31825ae6dc. Crit Care Med. 2012. PMID: 22903106 No abstract available.
-
Paediatrics: paediatric CRRT and ECMO: fluid overload is not the only issue.Nat Rev Nephrol. 2012 Oct;8(10):565-6. doi: 10.1038/nrneph.2012.193. Epub 2012 Sep 4. Nat Rev Nephrol. 2012. PMID: 22945486 No abstract available.
References
-
- Weber TR, Connors RH, Tracy TF, Jr, et al. Prognostic determinants in extracorporeal membrane oxygenation for respiratory failure in newborns. Ann Thorac Surg. 1990;50(5):720–723. - PubMed
-
- Heiss KF, Pettit B, Hirschl RB, et al. Renal insufficiency and volume overload in neonatal ECMO managed by continuous ultrafiltration. ASAIO Trans. 1987;33(3):557–560. - PubMed
-
- Kelly RE, Jr, Phillips JD, Foglia RP, et al. Pulmonary edema and fluid mobilization as determinants of the duration of ECMO support. J Pediatr Surg. 1991;26(9):1016–1022. - PubMed
-
- Smith AH, Hardison DC, Worden CR, et al. Acute renal failure during extracorporeal support in the pediatric cardiac patient. ASAIO J. 2009;55(4):412–416. - PubMed
-
- Swaniker F, Kolla S, Moler F, et al. Extracorporeal life support outcome for 128 pediatric patients with respiratory failure. J Pediatr Surg. 2000;35(2):197–202. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
