

Rare giant traumatic cervical arteriovenous fistula in neurofibromatosis type 1 patient
- PMID: 22744260
- PMCID: PMC3387472
- DOI: 10.1136/bcr.12.2011.5354
Rare giant traumatic cervical arteriovenous fistula in neurofibromatosis type 1 patient
Abstract
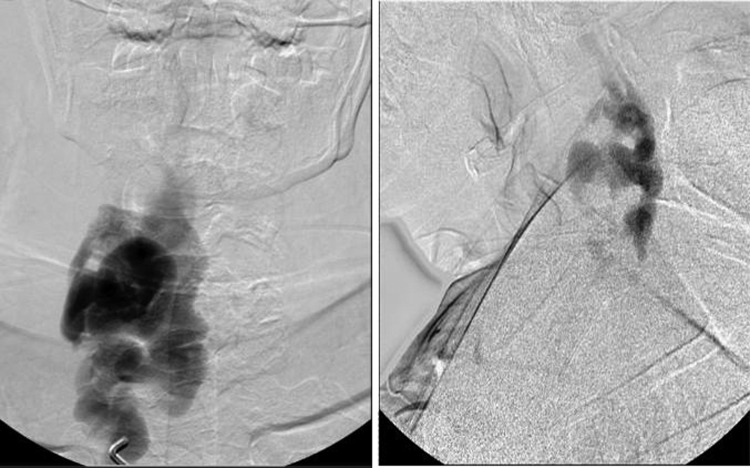
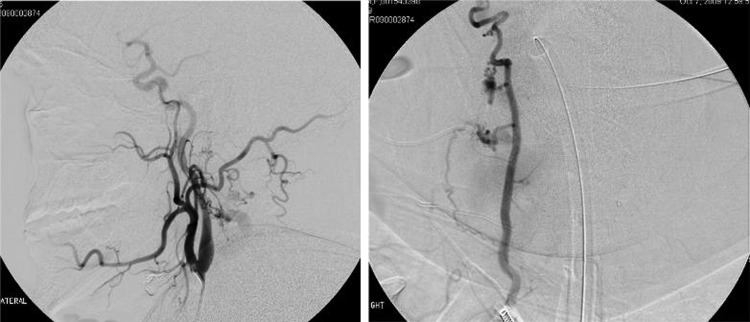
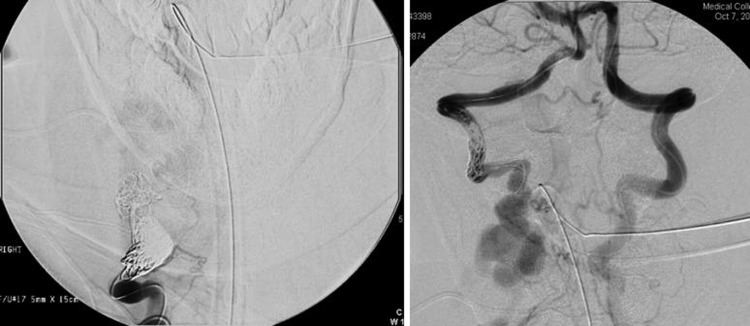
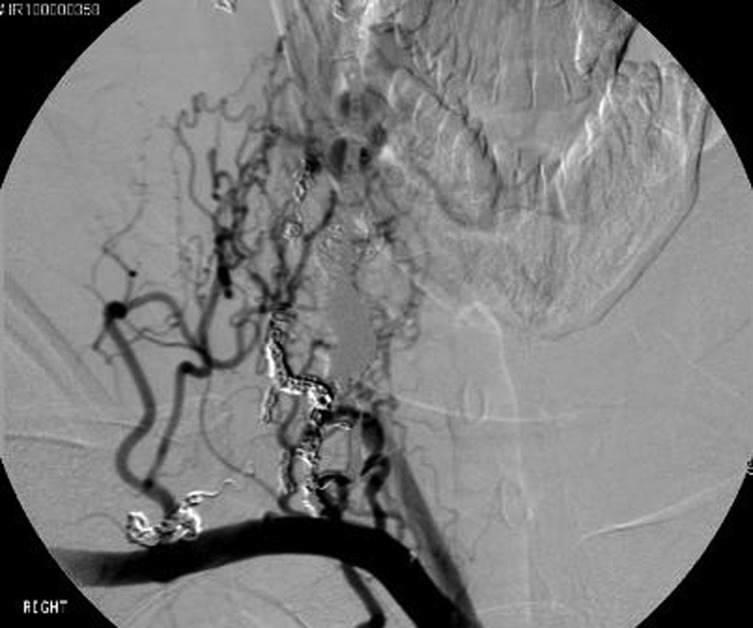
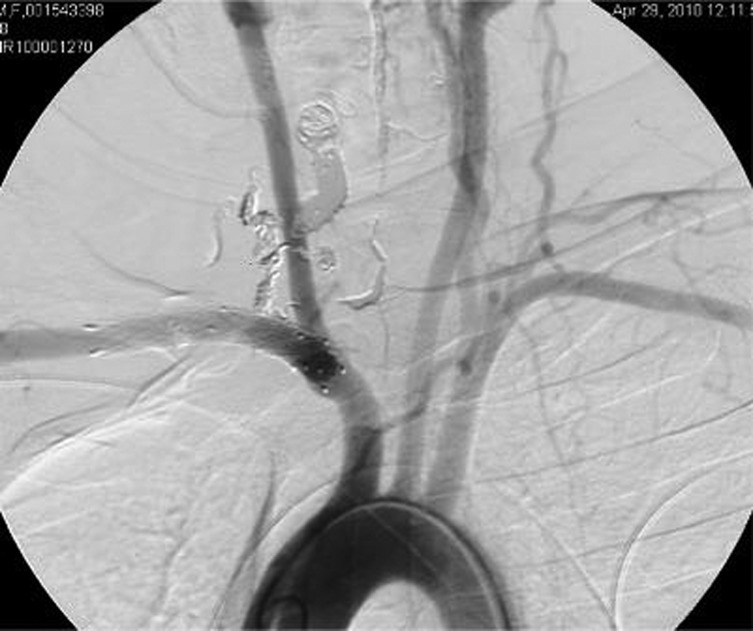
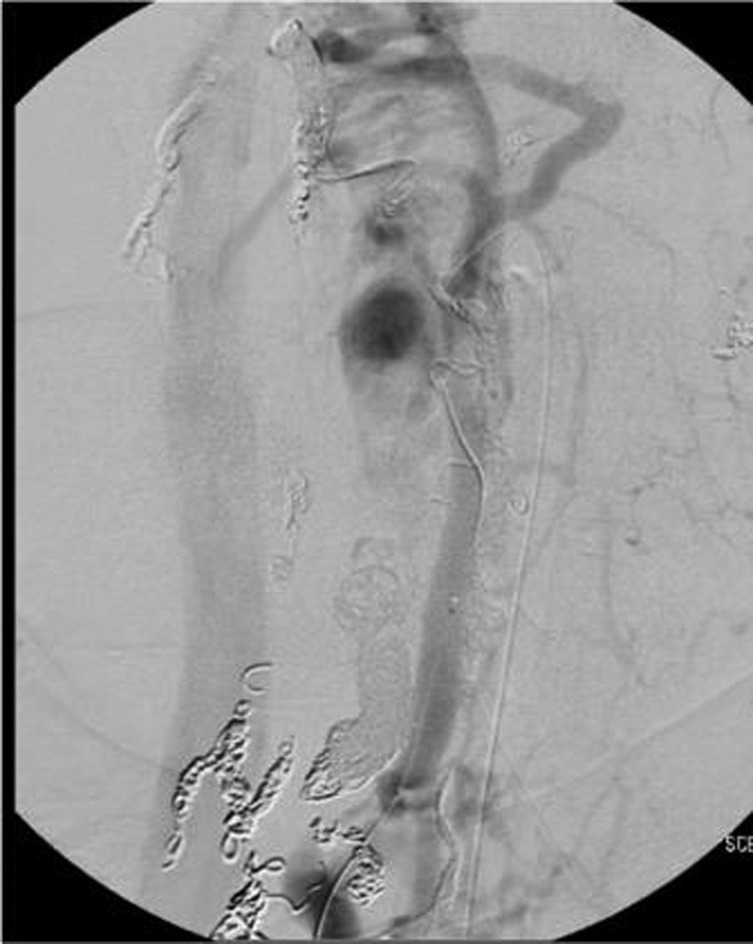
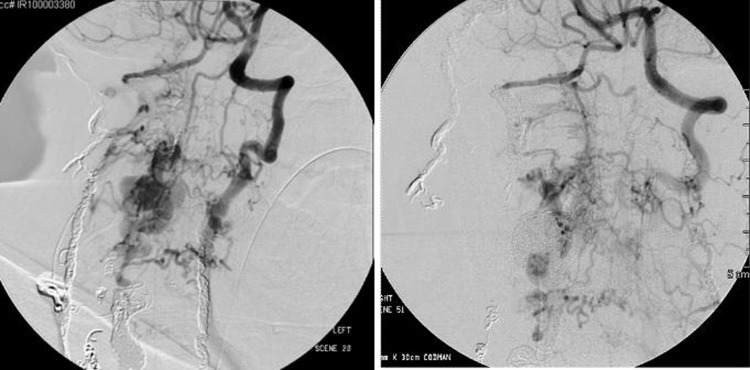
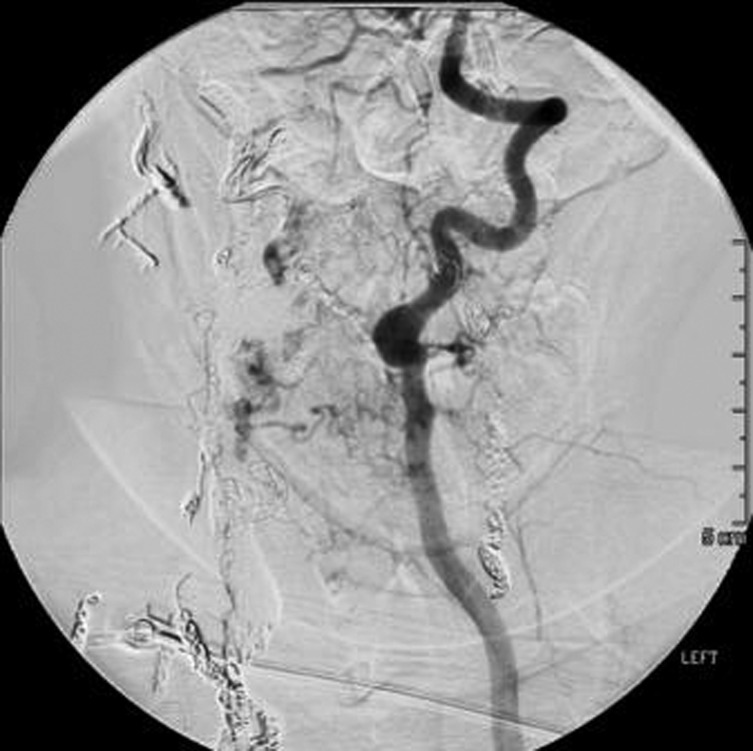
Arteriovenous fistulas can rarely occur in patients with neurofibromatosis type 1. These lesions typically result from traumatic insult to the dysplastic parent artery. The damaged artery forms abnormal connections with nearby paraspinal and epidural venous structures. Surgical treatment of these lesions can be extremely challenging given the proximity to the spinal cord and the ability of the fistula to recruit vessels from adjacent vascular structures. A 29-year-old woman with neurofibromatosis type 1 and a motor vehicle collision 2 years earlier presented with gait difficulty, lower extremity spasticity and neck and arm pain. Her investigation revealed a giant cervical vertebral arteriovenous fistula. The fistula was successfully treated in multiple stages using all endovascular techniques including detachable coils, stents and glue embolisation. Reduction in flow and improvement in symptoms are reasonable goals in this specific rare subgroup of complex cervical arteriovenous fistulae.
Conflict of interest statement
Figures
Similar articles
-
Combined transarterial and percutaneous coiling of a spontaneous vertebrovertebral fistula associated with neurofibromatosis Type 1. Case report.J Neurosurg. 2009 Jul;111(1):37-40. doi: 10.3171/2008.12.JNS081209. J Neurosurg. 2009. PMID: 19301970
-
Endovascular treatment for bilateral vertebral arteriovenous fistulas in neurofibromatosis 1.Australas Radiol. 2003 Dec;47(4):457-61. doi: 10.1046/j.1440-1673.2003.01221.x. Australas Radiol. 2003. PMID: 14641204
-
Vertebral arteriovenous fistulae (AVF) in neurofibromatosis type 1: a report of two cases.Turk Neurosurg. 2013;23(2):289-93. doi: 10.5137/1019-5149.JTN.4993-11.0. Turk Neurosurg. 2013. PMID: 23546922
-
[Symptomatic arteriovenous fistula in a patient with neurofibromatosis type I].No Shinkei Geka. 1997 Apr;25(4):373-8. No Shinkei Geka. 1997. PMID: 9125723 Review. Japanese.
-
Vertebral artery aneurysms and cervical arteriovenous fistulae in patients with neurofibromatosis 1.Vascular. 2010 May-Jun;18(3):166-77. doi: 10.2310/6670.2010.00032. Vascular. 2010. PMID: 20470689 Review.
Cited by
-
Neurovascular manifestations of connective-tissue diseases: A review.Interv Neuroradiol. 2016 Dec;22(6):624-637. doi: 10.1177/1591019916659262. Epub 2016 Aug 10. Interv Neuroradiol. 2016. PMID: 27511817 Free PMC article. Review.
-
Neurofibromatosis type 1 with subarachnoid haemorrhage from the left vertebral arteriovenous fistula: case presentation and literature review.BMJ Case Rep. 2021 Feb 22;14(2):e239880. doi: 10.1136/bcr-2020-239880. BMJ Case Rep. 2021. PMID: 33619142 Free PMC article. Review.
-
Paraspinal arteriovenous fistula: Stuttgart classification based on experience and a review of the literature.Br J Radiol. 2018 Jul;91(1088):20170337. doi: 10.1259/bjr.20170337. Epub 2018 Mar 2. Br J Radiol. 2018. PMID: 29376731 Free PMC article. Review.
-
Cervical spinal extradural arteriovenous fistula successfully treated using transarterial balloon-assisted coil embolization.J Cerebrovasc Endovasc Neurosurg. 2020 Sep;22(3):182-189. doi: 10.7461/jcen.2020.22.3.182. Epub 2020 Sep 21. J Cerebrovasc Endovasc Neurosurg. 2020. PMID: 32971577 Free PMC article.
References
-
- Deans WR, Bloch S, Leibrock L, et al. Arteriovenous fistula in patients with neurofibromatosis. Radiology 1982;144:103–7. - PubMed
-
- Saito A, Takahashi T, Ezura M, et al. Intercostal arteriovenous fistula associated with neurofibromatosis manifesting as congestive myelopathy: case report. Neurosurgery 2007;61:E656–7; discussion E657. - PubMed
-
- Schievink WI, Piepgras DG. Cervical vertebral artery aneurysms and arteriovenous fistulae in neurofibromatosis type 1: case reports. Neurosurgery 1991;29:760–5. - PubMed
-
- Chou SN, French LA. Arteriovenous fistula of vertebral vessels in the neck. J Neurosurg 1965;22:77–80. - PubMed
-
- Kāhārā V, Lehto U, Ryymin P, et al. Vertebral epidural arteriovenous fistula and radicular pain in neurofibromatosis type I. Acta Neurochir (Wien) 2002;144:493–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials