

Evaluation of CT angiography for visualisation of the lenticulostriate artery: difference between normotensive and hypertensive patients
- PMID: 22744324
- PMCID: PMC3500797
- DOI: 10.1259/bjr/67294268
Evaluation of CT angiography for visualisation of the lenticulostriate artery: difference between normotensive and hypertensive patients
Abstract
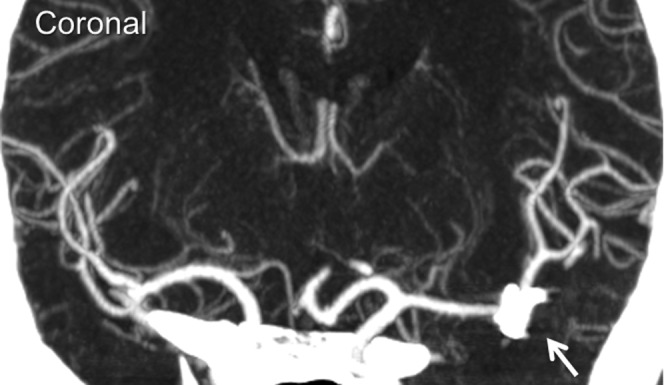
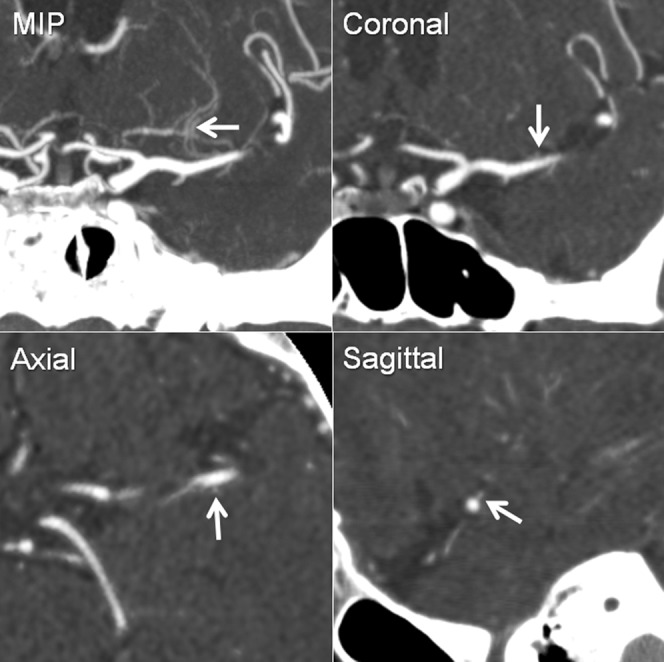
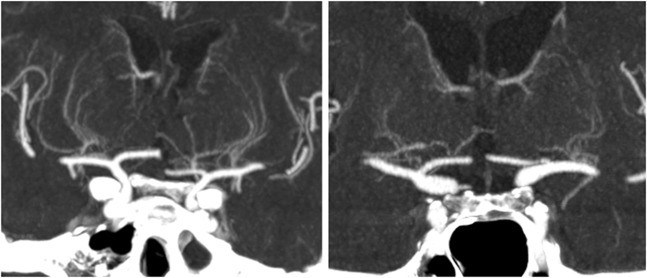
Objective: High-resolution CT angiography (CTA) is currently available using multidetector row CT (MDCT); however, its use for small artery visualisation has been limited. To evaluate its capability, we investigated CTA visualisation for difference in number of the lenticulostriate artery (LSA) branches between normotensive and hypertensive patients, because hypertension is a major cause of LSA damage.
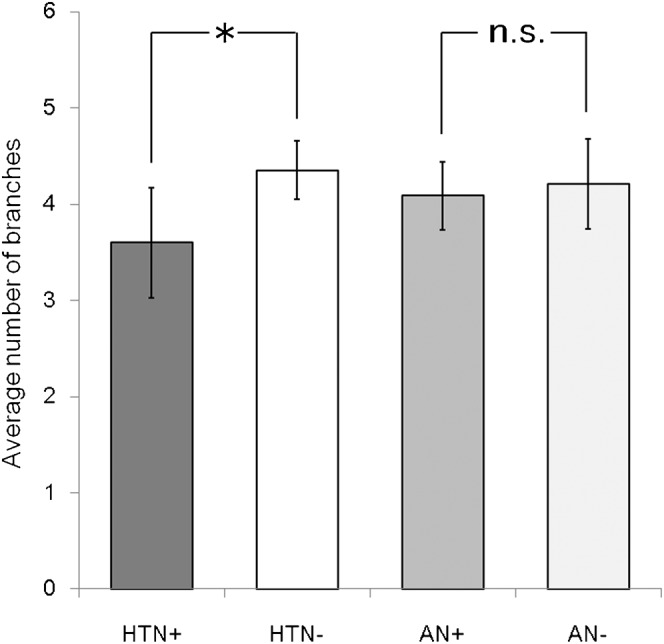
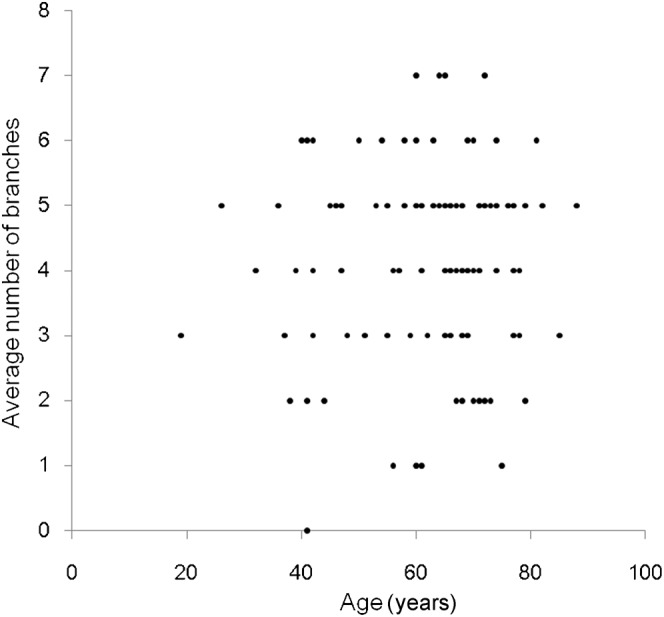
Methods: This was a retrospective study evaluating cerebrovascular CTA at our hospital conducted from February 2008 to June 2009 under approval of the institutional review board. 117 patients (39 males and 78 females, 19-88 years old) were included. CTA was conducted using a 64 channel MDCT. Total numbers of LSA branches were examined for differences by age with regression analysis and the presence or absence of hypertension and/or aneurysm using two-sample t-tests. A p-value <0.016 was considered statistically significant after correction for multiple comparisons. A multiple variable analysis of three factors was also conducted.
Results: The average number of LSA branches was 3.6 [95% confidence interval (CI) 3.0-4.1] and 4.4 (95% CI 4.1-4.7), respectively, for a patient with and without history of hypertension, and the difference was statistically significant (p=0.013). The difference was approximately one branch in the multiple variable analysis. No significant correlation was observed for age and no significant difference was observed for the presence or absence of aneurysms.
Conclusions: Contrast-enhanced CTA can visualise significant differences in the number of LSA branches among patients with and without hypertension. Advances in knowledge Current high-resolution CTA can visualise LSA well, which enables finding a difference in the LSA between normotensive subjects and hypertensive patients.
Figures
Similar articles
-
Evaluation of renal artery in hypertensive patients by unenhanced MR angiography using spatial labeling with multiple inversion pulses sequence and by CT angiography.AJR Am J Roentgenol. 2012 Nov;199(5):1142-8. doi: 10.2214/AJR.11.7263. AJR Am J Roentgenol. 2012. PMID: 23096191
-
Hypertension correlates with lenticulostriate arteries visualized by 7T magnetic resonance angiography.Hypertension. 2009 Nov;54(5):1050-6. doi: 10.1161/HYPERTENSIONAHA.109.140350. Epub 2009 Oct 5. Hypertension. 2009. PMID: 19805635
-
Visualization of lenticulostriate arteries by flow-sensitive black-blood MR angiography on a 1.5 T MRI system: a comparative study between subjects with and without stroke.AJNR Am J Neuroradiol. 2013 Apr;34(4):780-4. doi: 10.3174/ajnr.A3310. Epub 2012 Oct 11. AJNR Am J Neuroradiol. 2013. PMID: 23064597 Free PMC article. Clinical Trial.
-
Lenticulostriate aneurysms: a case series and review of the literature.J Neurointerv Surg. 2015 Mar;7(3):194-201. doi: 10.1136/neurintsurg-2013-010969. Epub 2014 Feb 26. J Neurointerv Surg. 2015. PMID: 24574545 Review.
-
Can computed tomography angiography of the brain replace lumbar puncture in the evaluation of acute-onset headache after a negative noncontrast cranial computed tomography scan?Acad Emerg Med. 2010 Apr;17(4):444-51. doi: 10.1111/j.1553-2712.2010.00694.x. Acad Emerg Med. 2010. PMID: 20370785 Review.
Cited by
-
Vessel density mapping of small cerebral vessels on 3D high resolution black blood MRI.Neuroimage. 2024 Feb 1;286:120504. doi: 10.1016/j.neuroimage.2023.120504. Epub 2024 Jan 11. Neuroimage. 2024. PMID: 38216104 Free PMC article.
-
Parent artery occlusion for unruptured cerebral aneurysms: the Japanese Registry of Neuroendovascular Therapy (JR-NET) 1 and 2.Neurol Med Chir (Tokyo). 2014;54(2):91-7. doi: 10.2176/nmc.oa2013-0185. Epub 2013 Dec 5. Neurol Med Chir (Tokyo). 2014. PMID: 24305030 Free PMC article.
-
High-resolution cone beam CT for evaluation of vascular channel in intracranial partial thrombosed aneurysm.Nagoya J Med Sci. 2018 May;80(2):279-284. doi: 10.18999/nagjms.80.2.279. Nagoya J Med Sci. 2018. PMID: 29915445 Free PMC article.
-
Deep learning-based 3D cerebrovascular segmentation workflow on bright and black blood sequences magnetic resonance angiography.Insights Imaging. 2024 Mar 22;15(1):81. doi: 10.1186/s13244-024-01657-0. Insights Imaging. 2024. PMID: 38517610 Free PMC article.
-
Porto Alegre Line predicts lenticulostriate arteries encasement and extent of resection in insular gliomas. A preliminary study.Front Surg. 2025 Feb 10;12:1414302. doi: 10.3389/fsurg.2025.1414302. eCollection 2025. Front Surg. 2025. PMID: 39996150 Free PMC article.
References
-
- Marinkovic SV, Gibo H. The surgical anatomy of the perforating branches of the basilar artery. Neurosurgery 1993;33:80–7 - PubMed
-
- Greenberg SM. Small vessels, big problems. N Engl J Med 2006;354:1451–3 - PubMed
-
- Wardlaw JM, Dennis MS, Warlow CP, Sandercock PA. Imaging appearance of the symptomatic perforating artery in patients with lacunar infarction: occlusion or other vascular pathology? Ann Neurol 2001;50:208–15 - PubMed
-
- Feekes JA, Cassell MD. The vascular supply of the functional compartments of the human striatum. Brain 2006;129:2189–201 - PubMed
-
- Caplan LR. Intracranial branch atheromatous disease: a neglected, understudied, and underused concept. Neurology 1989;39:1246–50 - PubMed
