

Progress in the management of patients with uveal melanoma. The 2012 Ashton Lecture
- PMID: 22744385
- PMCID: PMC3443832
- DOI: 10.1038/eye.2012.126
Progress in the management of patients with uveal melanoma. The 2012 Ashton Lecture
Abstract
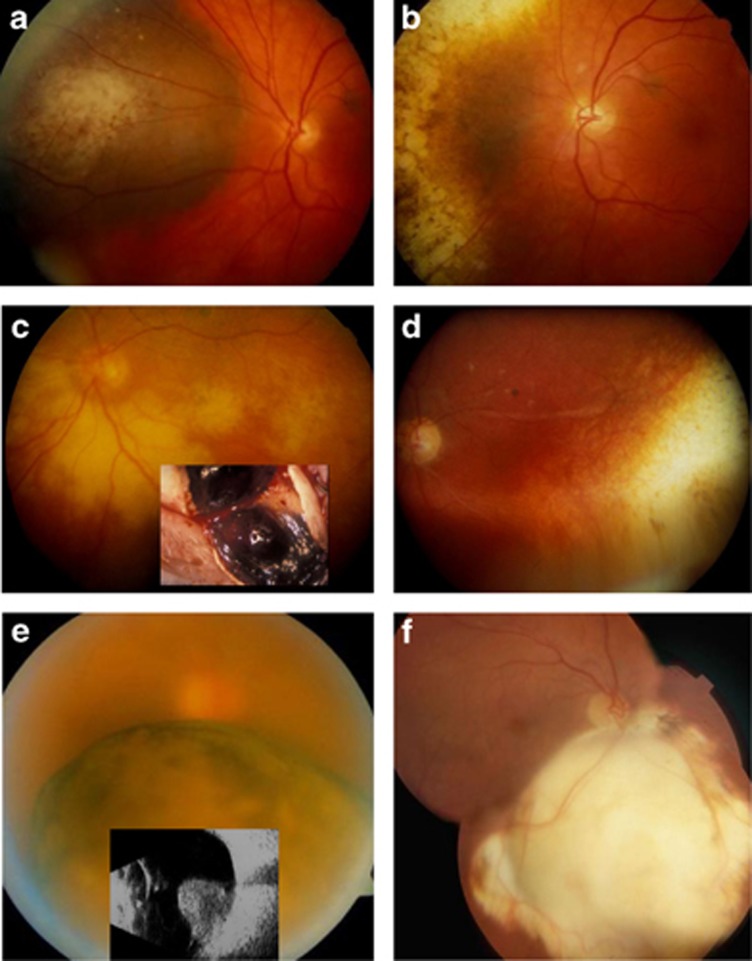
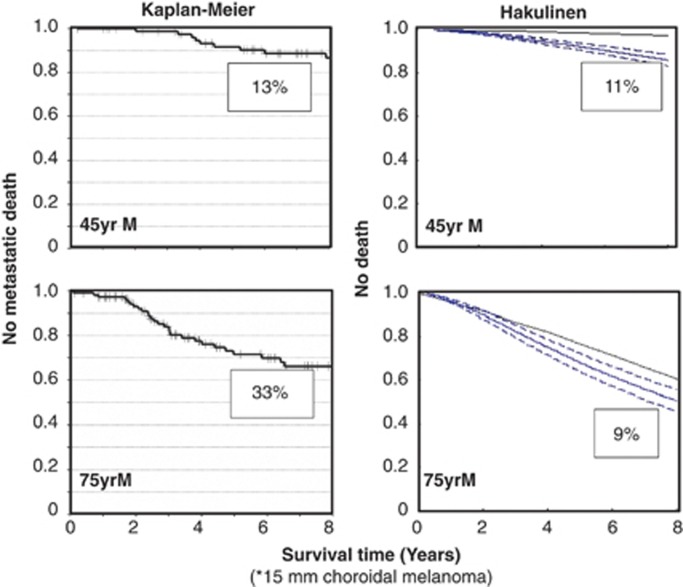
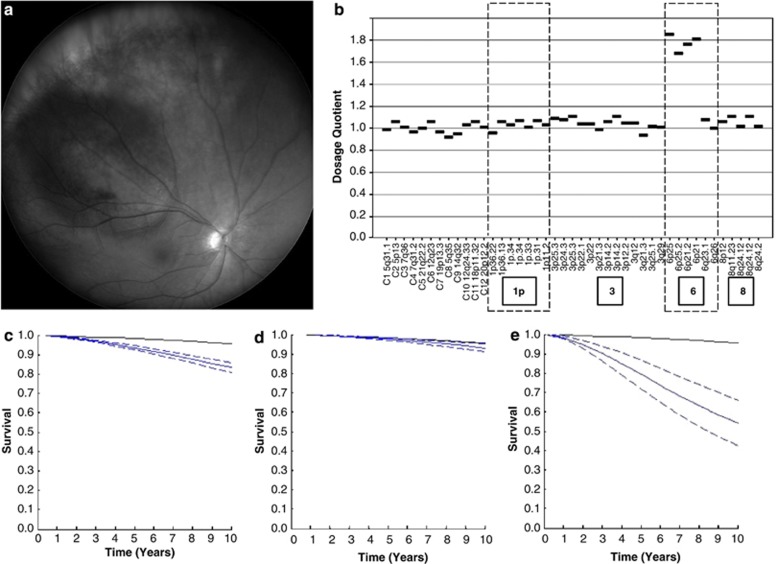
Uveal melanomas are diverse in their clinical features and behaviour. More than 90% involve the choroid, the remainder being confined to the ciliary body and iris. Most patients experience visual loss and more than a third require enucleation, in some cases because of pain. Diagnosis is based on slit-lamp biomicroscopy and/or ophthalmoscopy, with ultrasonography, autofluorescence photography, and/or biopsy in selected cases. Conservation of the eye with useful vision has improved with advances in brachytherapy, proton beam radiotherapy, endoresection, exoresection, transpupillary thermotherapy, and photodynamic therapy. Despite ocular treatment, almost 50% of patients develop metastatic disease, which occurs almost exclusively in patients whose tumour shows chromosome 3 loss and/or class 2 gene expression profile. When the tumour shows such lethal genetic changes, the survival time depends on the anatomical stage and the histological grade of malignancy. Prognostication has improved as a result of progress in multivariate analysis including all the major risk factors. Screening for metastases is more sensitive as a consequence of advances in liver scanning with magnetic resonance imaging and other methods. More patients with metastases are living longer, benefiting from therapies such as: partial hepatectomy; radiofrequency ablation; ipilumumab immunotherapy; selective internal radiotherapy; intra-hepatic chemotherapy, possibly with isolated liver perfusion; and systemic chemotherapy. There is scope for improvement in the detection of uveal melanoma so as to maximise any opportunities for conserving the eye and vision, as well as preventing metastatic spread. Patient management has been enhanced by the formation of multidisciplinary teams in specialised ocular oncology centres.
Figures
References
-
- Damato BE, Foulds WS. Tumour-associated retinal pigment epitheliopathy. Eye. 1990;4:382–387. - PubMed
-
- Coupland SE, Campbell I, Damato B. Routes of extraocular extension of uveal melanoma: risk factors and influence on survival probability. Ophthalmology. 2008;115:1778–1785. - PubMed
-
- Eskelin S, Pyrhönen S, Hahka-Kemppinen M, Tuomaala S, Kivelä T. A prognostic model and staging for metastatic uveal melanoma. Cancer. 2003;97:465–475. - PubMed
