

Dose intensification of daunorubicin and cytarabine during treatment of adult acute lymphoblastic leukemia: results of Cancer and Leukemia Group B Study 19802
- PMID: 22744771
- PMCID: PMC4220742
- DOI: 10.1002/cncr.27617
Dose intensification of daunorubicin and cytarabine during treatment of adult acute lymphoblastic leukemia: results of Cancer and Leukemia Group B Study 19802
Erratum in
- Cancer. 2014 Jul 15;120(14):2222. Dosage error in article text.
-
Erratum: Stock W, Johnson JL, Stone RM, Kolitz JE, Powell BL, Wetzler M, Westervelt P, Marcucci G, DeAngelo DJ, Vardiman JW, McDonnell D, Mrózek K, Bloomfield CD and Larson R A. Dose intensification of daunorubicin and cytarabine during treatment of adult acute lymphoblastic leukemia. Cancer. 2013;119:90-8.Cancer. 2014 Jul 15;120(14):2222. doi: 10.1002/cncr.28708. Epub 2014 Apr 3. Cancer. 2014. PMID: 26437204 No abstract available.
Abstract
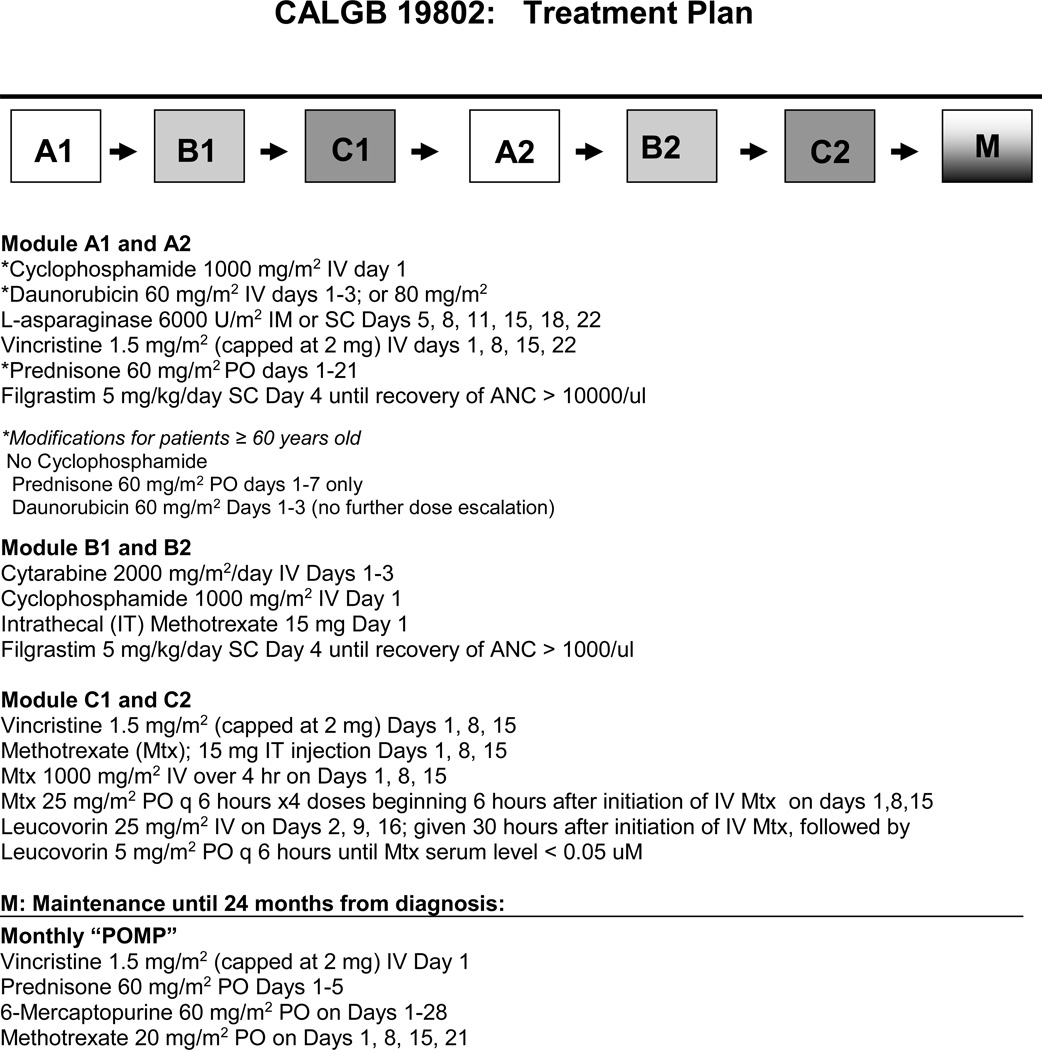
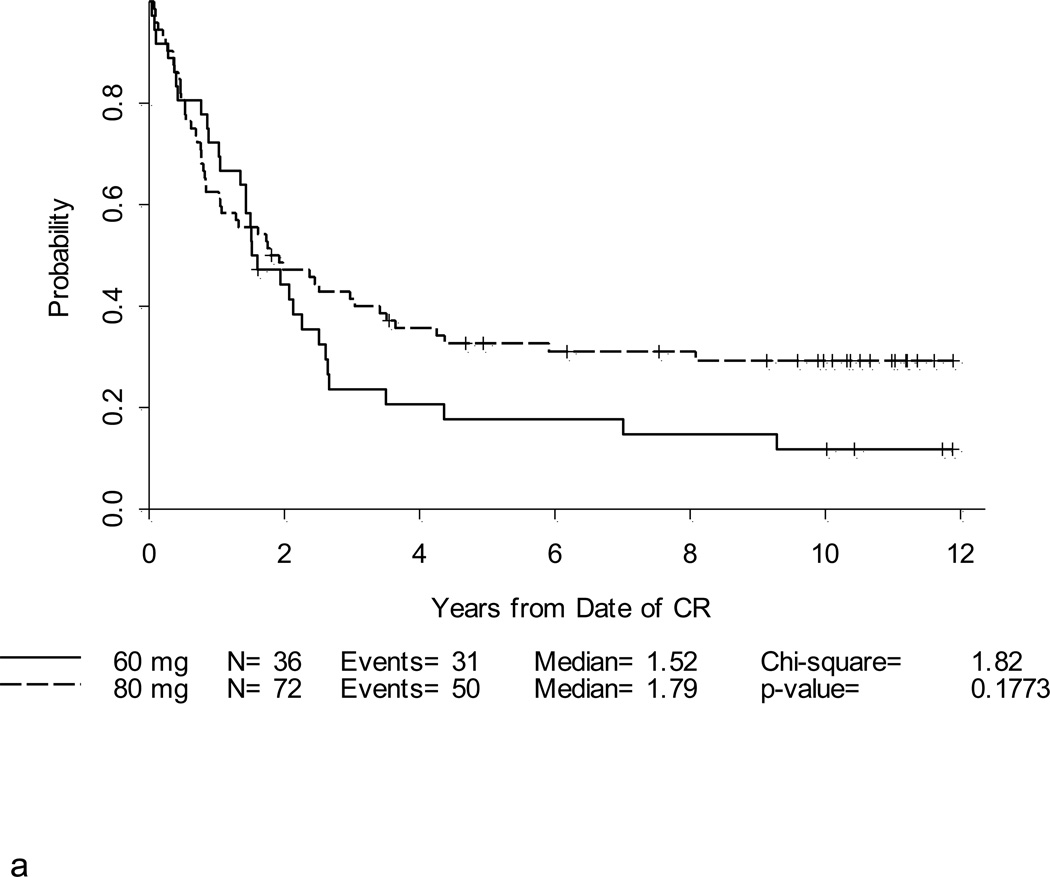
Background: Cancer and Leukemia Group B (CALGB) Study 19802, a phase 2 study, evaluated whether dose intensification of daunorubicin and cytarabine could improve disease-free survival (DFS) in adults with acute lymphoblastic leukemia (ALL) and whether high-dose systemic and intrathecal methotrexate could replace cranial radiotherapy for central nervous system (CNS) prophylaxis.
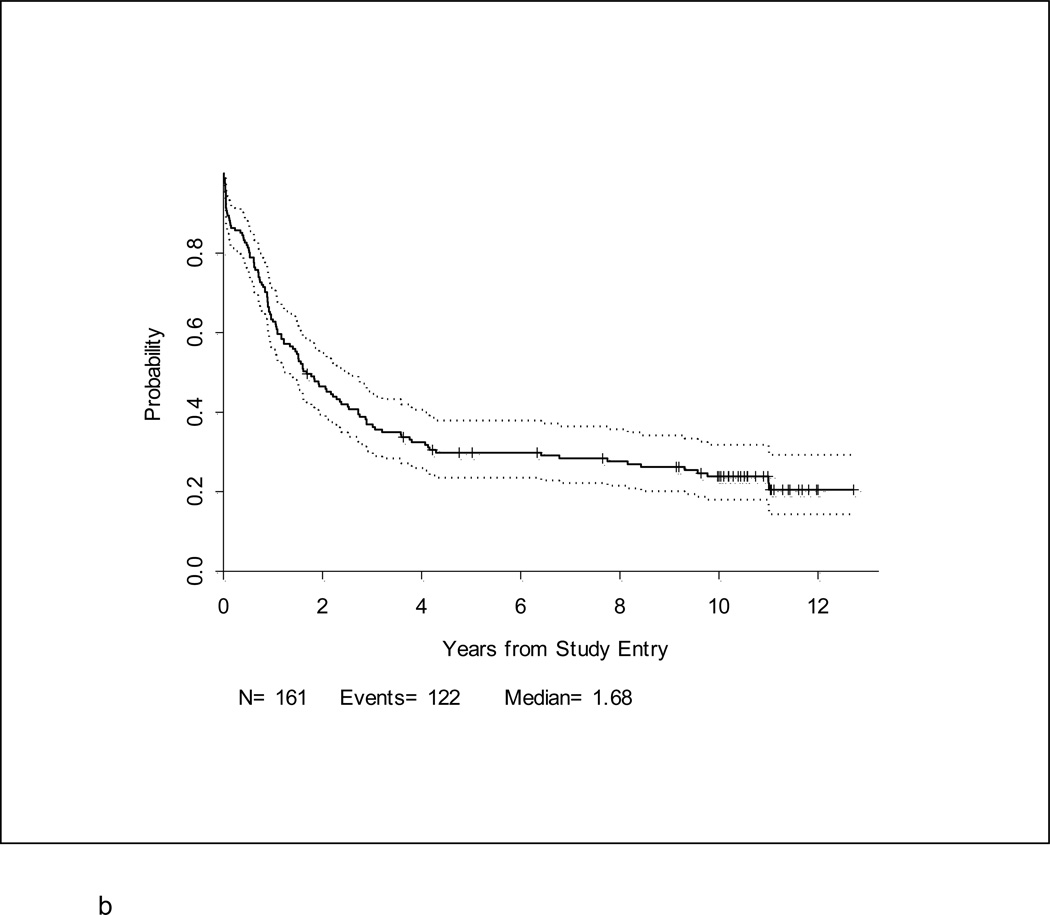
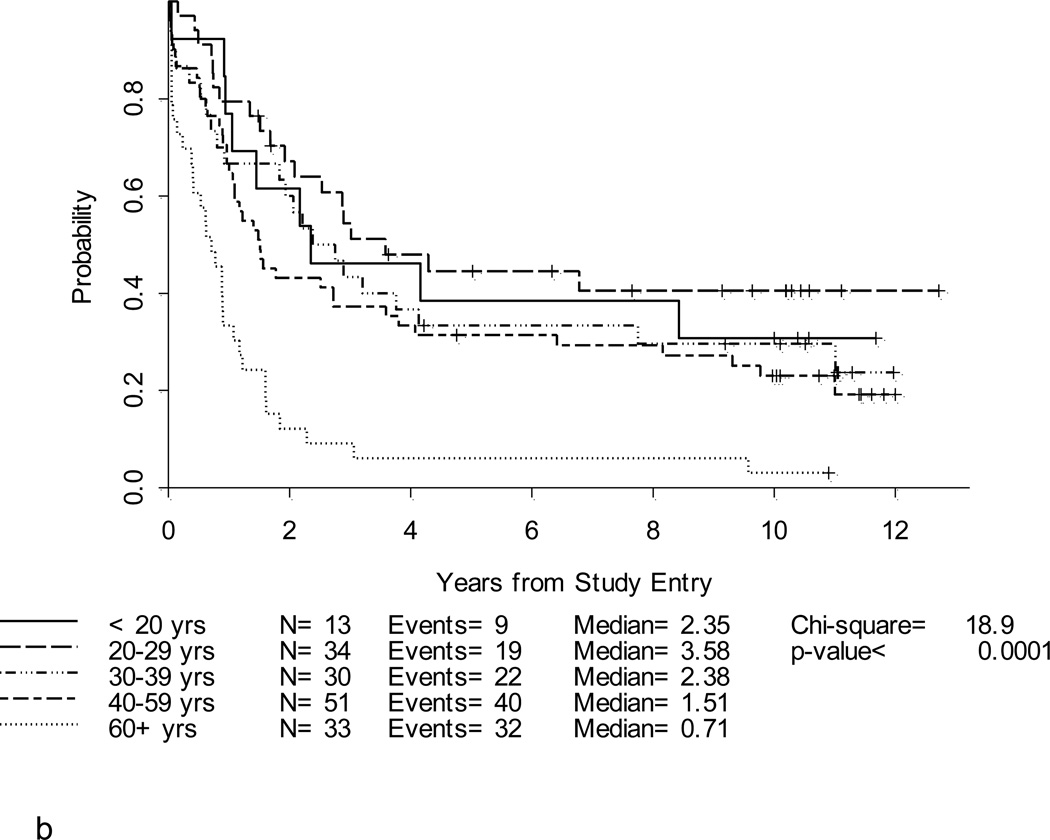
Methods: One hundred sixty-one eligible, previously untreated patients ages 16 to 82 years (median age, 40 years) were enrolled, and 33 (20%) were aged ≥60 years.
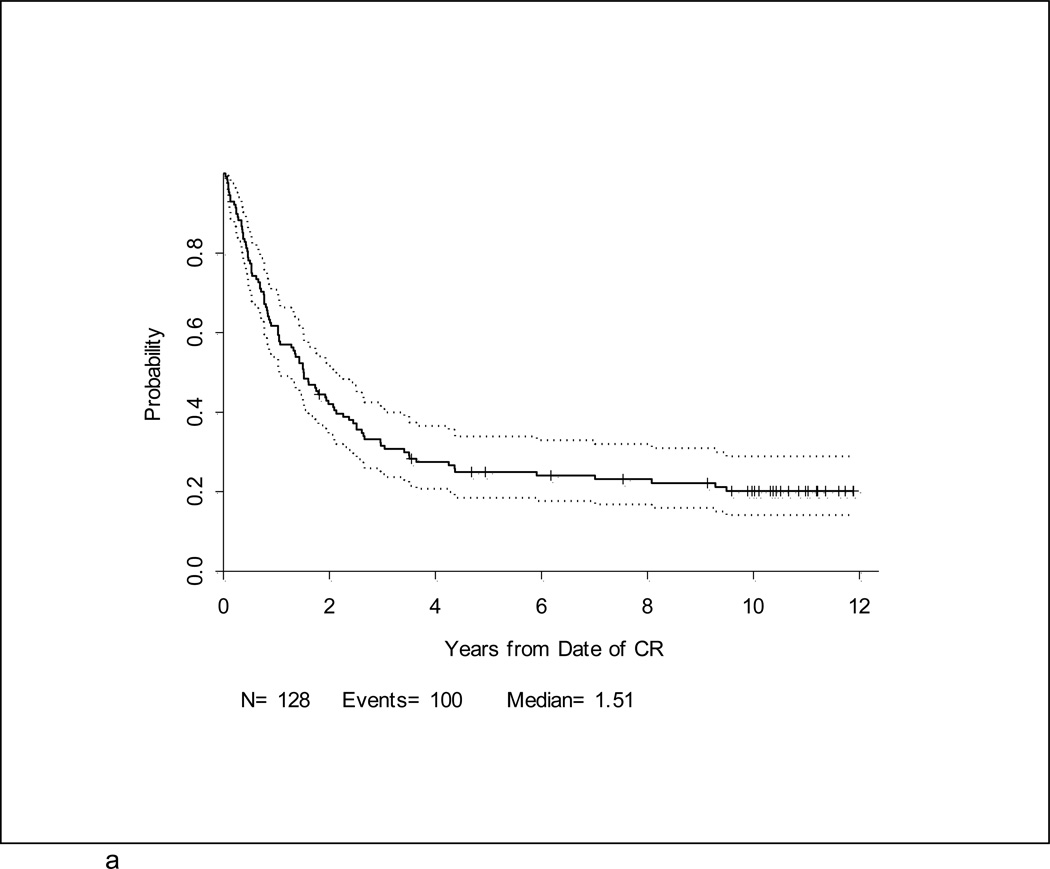
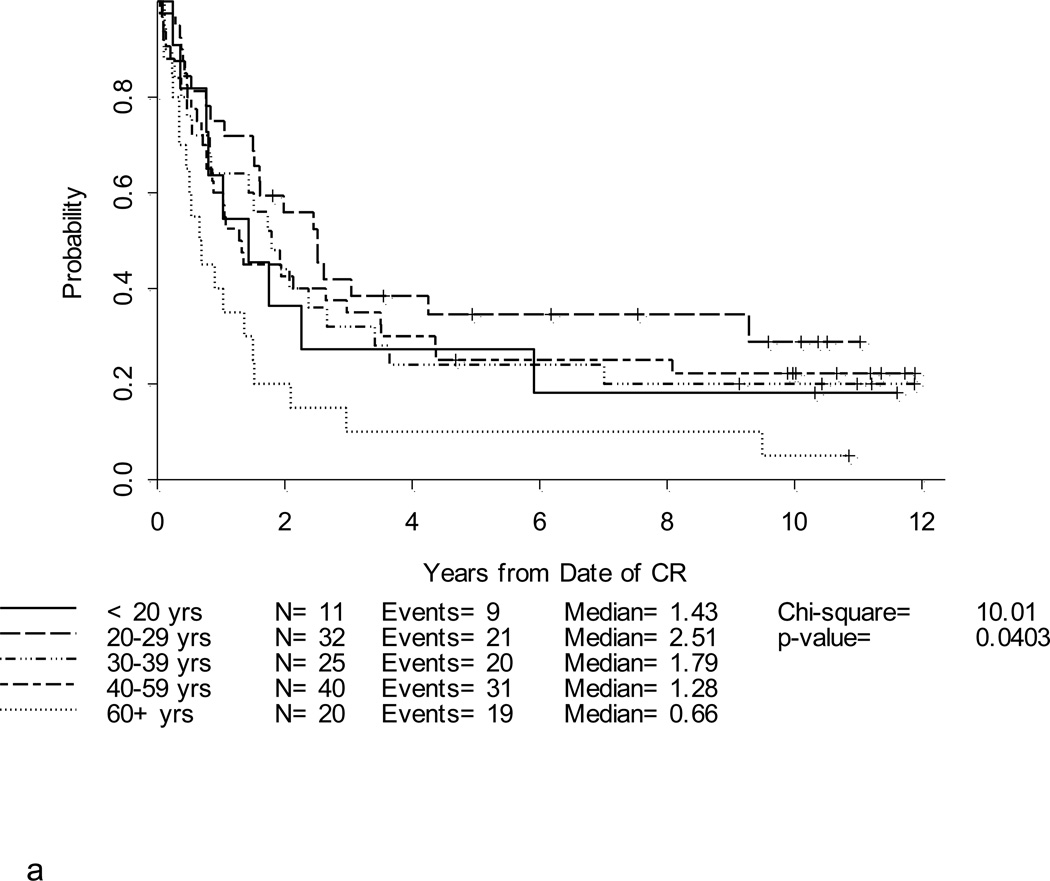
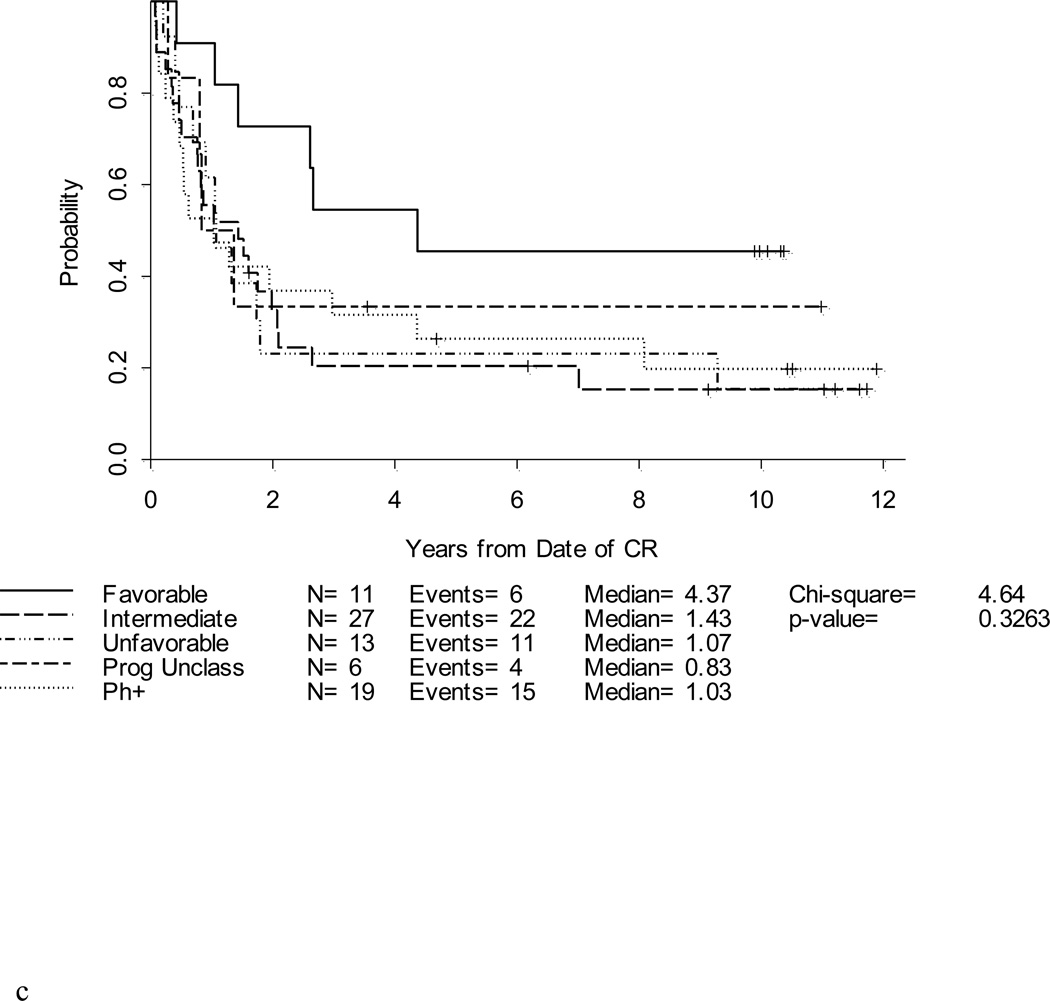
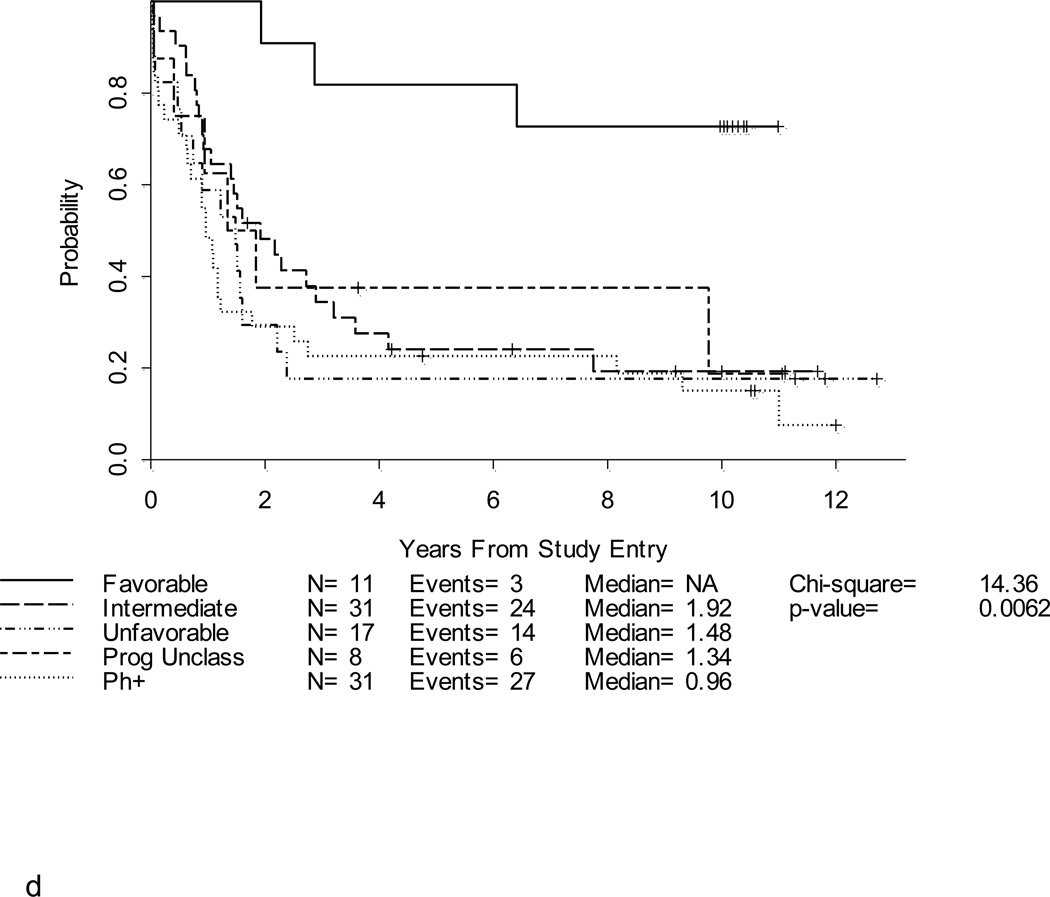
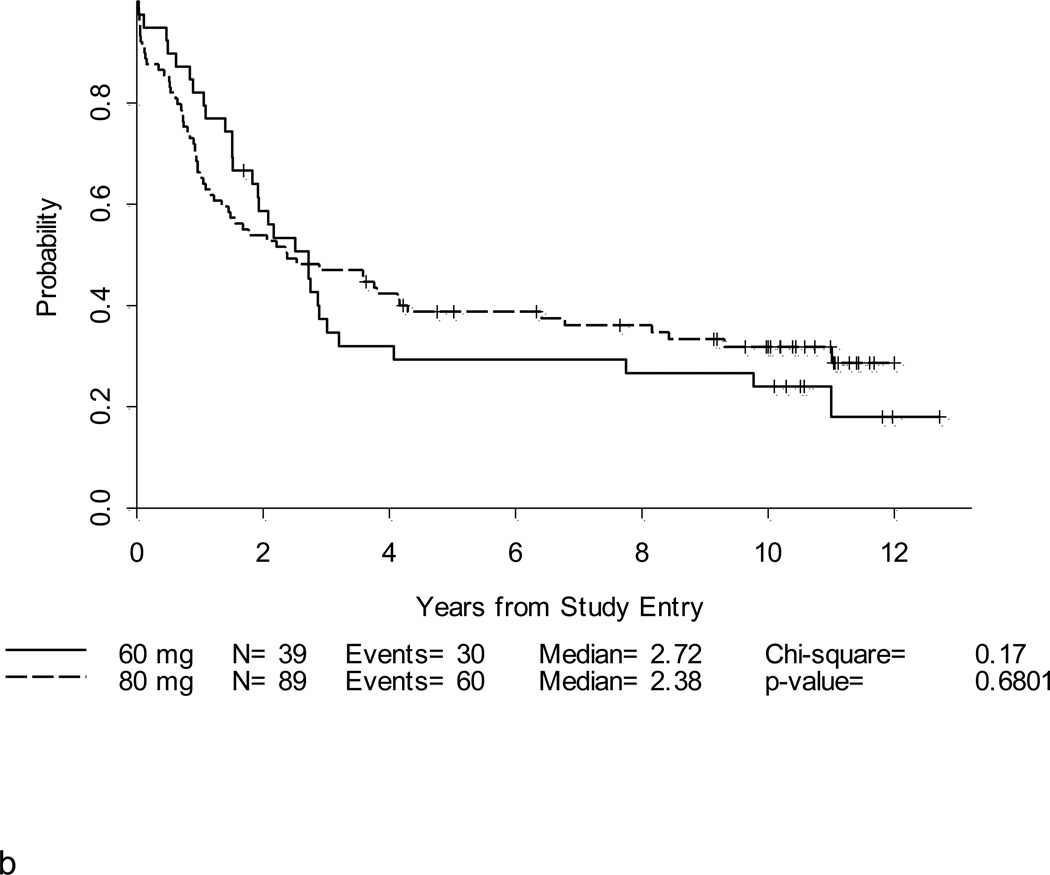
Results: One hundred twenty-eight patients (80%) achieved complete remission (CR). Dose intensification of daunorubicin and cytarabine was feasible. At a median follow-up of 10.4 years for surviving patients, the 5-year DFS rate was 25% (95% confidence interval, 18%-33%), and the overall survival (OS) rate was 30% (95% confidence interval, 23%-37%). Patients aged <60 years who received the 80 mg/m(2) dose of daunorubicin had a DFS of 33% (95% confidence interval, 22%-44%) and an OS of 39% (95% confidence interval, 29%-49%) at 5 years. Eighty-four patients (52%) relapsed, including 9 patients (6%) who had isolated CNS relapses. The omission of cranial irradiation did not result in higher than historic CNS relapse rates.
Conclusions: Intensive systemic, oral, and intrathecal methotrexate dosing permitted the omission of CNS irradiation in adult patients with ALL. This intensive approach using higher doses of daunorubicin and cytarabine failed to result in an overall improvement in DFS or OS compared with historic CALGB studies. Future therapeutic strategies for adults with ALL should be tailored to specific age and molecular genetic subsets.
Copyright © 2012 American Cancer Society.
Figures
References
-
- Bassan R, Pogliani E, Casula P, et al. Risk-oriented postremission strategies in adult acute lymphoblastic leukemia: prospective confirmation of anthracycline activity in standard-risk class and role of hematopoietic stem cell transplants in high-risk groups. Hematol J. 2001;2(2):117–126. - PubMed
-
- Gokbuget N, Hoelzer D, Arnold R, et al. Treatment of Adult ALL according to protocols of the German Multicenter Study Group for Adult ALL (GMALL) Hematol Oncol Clin North Am. 2000 Dec;14(6):1307–1325. ix. - PubMed
-
- Hofmann WK, Seipelt G, Langenhan S, et al. Prospective randomized trial to evaluate two delayed granulocyte colony stimulating factor administration schedules after high-dose cytarabine therapy in adult patients with acute lymphoblastic leukemia. Ann Hematol. 2002 Oct;81(10):570–574. - PubMed
-
- Kantarjian H, Thomas D, O'Brien S, et al. Long-term follow-up results of hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone (Hyper-CVAD), a dose-intensive regimen, in adult acute lymphocytic leukemia. Cancer. 2004 Dec 15;101(12):2788–2801. - PubMed
-
- Larson RA. The U.S. trials in adult acute lymphoblastic leukemia. Ann Hematol. 2004;83(Suppl 1):S127–S128. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U10 CA032291/CA/NCI NIH HHS/United States
- CA33601/CA/NCI NIH HHS/United States
- CA02599/CA/NCI NIH HHS/United States
- CA32291/CA/NCI NIH HHS/United States
- U10 CA033601/CA/NCI NIH HHS/United States
- U10 CA180821/CA/NCI NIH HHS/United States
- CA35279/CA/NCI NIH HHS/United States
- P30 CA012197/CA/NCI NIH HHS/United States
- U10 CA101140/CA/NCI NIH HHS/United States
- CA77658/CA/NCI NIH HHS/United States
- CA101140/CA/NCI NIH HHS/United States
- U10 CA077658/CA/NCI NIH HHS/United States
- CA41287/CA/NCI NIH HHS/United States
- U10 CA035279/CA/NCI NIH HHS/United States
- CA03927/CA/NCI NIH HHS/United States
- U10 CA031946/CA/NCI NIH HHS/United States
- UG1 CA189850/CA/NCI NIH HHS/United States
- U10 CA041287/CA/NCI NIH HHS/United States
- CA31946/CA/NCI NIH HHS/United States
- U10 CA003927/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
