

Use of an atrial lead with very short tip-to-ring spacing avoids oversensing of far-field R-wave
- PMID: 22745661
- PMCID: PMC3382193
- DOI: 10.1371/journal.pone.0038277
Use of an atrial lead with very short tip-to-ring spacing avoids oversensing of far-field R-wave
Abstract
Objective: The AVOID-FFS (Avoidance of Far-Field R-wave Sensing) study aimed to investigate whether an atrial lead with a very short tip-to-ring spacing without optimization of pacemaker settings shows equally low incidence of far-field R-wave sensing (FFS) when compared to a conventional atrial lead in combination with optimization of the programming.
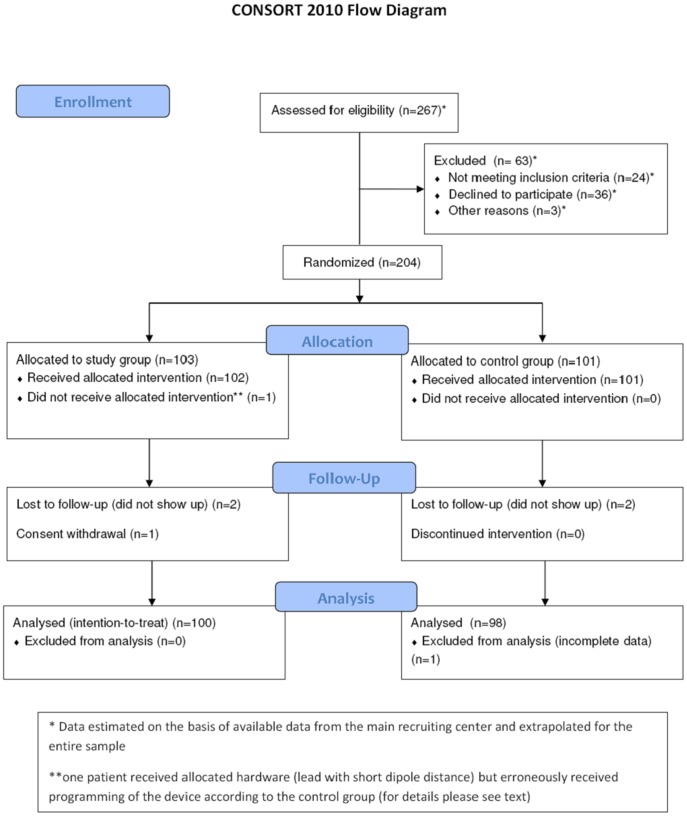
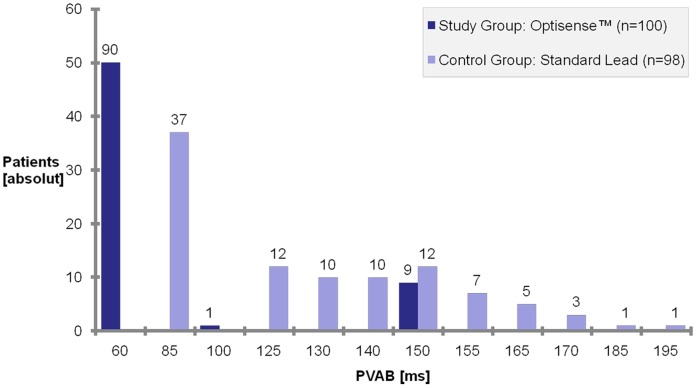
Methods: Patients receiving a dual chamber pacemaker were randomly assigned to receive an atrial lead with a tip-to-ring spacing of 1.1 mm or a lead with a conventional tip-to-ring spacing of 10 mm. Postventricular atrial blanking (PVAB) was programmed to the shortest possible value of 60 ms in the study group, and to an individually determined optimized value in the control group. Atrial sensing threshold was programmed to 0.3 mV in both groups. False positive mode switch caused by FFS was evaluated at one and three months post implantation.
Results: A total of 204 patients (121 male; age 73±10 years) were included in the study. False positive mode switch caused by FFS was detected in one (1%) patient of the study group and two (2%) patients of the control group (p = 0.62).
Conclusion: The use of an atrial electrode with a very short tip-to-ring spacing avoids inappropriate mode switch caused by FFS without the need for individual PVAB optimization.
Trial registration: ClinicalTrials.gov NCT00512915.
Conflict of interest statement
Figures

References
-
- Fitts SM, Hill MR, Mehra R, Gillis AM. High rate atrial tachyarrhythmia detections in implantable pulse generators: low incidence of false-positive detections. The PA Clinical Trial Investigators. Pacing Clin Electrophysiol. 2000;23:1080–6. - PubMed
-
- Pürerfellner H, Gillis AM, Holbrook R, Hettrick DA. Accuracy of atrial tachyarrhythmia detection in implantable devices with arrhythmia therapies. Pacing Clin Electrophysiol. 2004;27:983–92. - PubMed
-
- De Voogt WG, van Hemel NM, van de Bos AA, Koistinen J, Fast JH. Verification of pacemaker automatic mode switching for the detection of atrial fibrillation and atrial tachycardia with Holter recording. Europace. 2006;8:950–61. - PubMed
-
- Glotzer TV, Hellkamp AS, Zimmerman J, Sweeney MO, Yee R, et al. Atrial high rate episodes detected by pacemaker diagnostics predict death and stroke. Circulation. 2003;107:1614–9. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
