

The placenta in preeclampsia
- PMID: 22745921
- PMCID: PMC3381433
- DOI: 10.1016/j.preghy.2012.01.001
The placenta in preeclampsia
Abstract
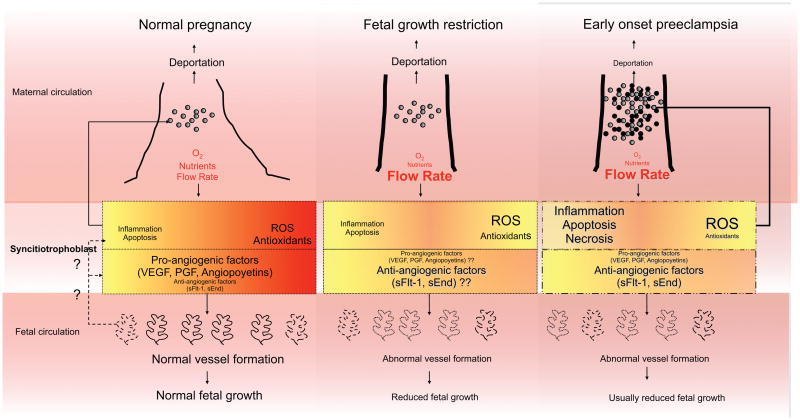
The root cause of preeclampsia is the placenta. Preeclampsia begins to abate with the delivery of the placenta and can occur in the absence of a fetus but with the presence of trophoblast tissue with hydatidiform moles. In view of this, study of the placenta should provide insight into the pathophysiology of preeclampsia. In this presentation we examine placental pathological and pathophysiological changes with preeclampsia and fetal growth restriction (FGR). It would seem that this comparison should be illuminating as both conditions are associated with similarly abnormal placentation yet only in preeclampsia is there a maternal pathophysiological syndrome. Similar insights about early and late onset preeclampsia should also be provided by such information.We report that the placental abnormalities in preeclampsia are what would be predicted in a setting of reduced perfusion and oxidative stress. However, the differences from FGR are inconsistent. The most striking differences between the two conditions are found in areas that have been the least studied. There are differences between the placental findings in early and late onset preeclampsia but whether these are qualitative, indicating different diseases, or simply quantitative differences within the same disease is difficult to determine.We attempt to decipher the true differences, seek an explanation for the disparate results and provide recommendations that we hope may help resolve these issues in future studies.
Figures
References
-
- Lain KY, Roberts JM. Contemporary concepts of the pathogenesis and management of preeclampsia.[comment] Journal of the American Medical Association. 2002;287(24):3183–6. - PubMed
-
- Roberts JM, Gammill HS. Preeclampsia: recent insights. Hypertension. 2005 Dec;46(6):1243–9. - PubMed
-
- Roberts J. Pregnancy related hypertension. In: Creasy R, Resnik R, Iams JD, editors. Maternal-Fetal Medicine: Principles and Practice. 6. Philadelphia: Saunders Elsevier; 2009. pp. 650–88.
-
- Brosens IA, Robertson WB, Dixon HG. The role of the spiral arteries in the pathogenesis of preeclampsia. In: Wynn R, editor. Obstetrics and Gynecology Annual. 1979. pp. 177–91. - PubMed
-
- Granger J, Alexander B, Abram S, Reckelhoff J, Wilson J, Rinewalt N. Chronic reductions in uterine perfusion pressure in the pregnant rat produces hypertension and reduces pressure- natriuresis. Hypertension. 2001 Mar;37(3):1013.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
