

Physical therapies for Achilles tendinopathy: systematic review and meta-analysis
- PMID: 22747701
- PMCID: PMC3537637
- DOI: 10.1186/1757-1146-5-15
Physical therapies for Achilles tendinopathy: systematic review and meta-analysis
Abstract
Background: Achilles tendinopathy (AT) is a common condition, causing considerable morbidity in athletes and non-athletes alike. Conservative or physical therapies are accepted as first-line management of AT; however, despite a growing volume of research, there remains a lack of high quality studies evaluating their efficacy. Previous systematic reviews provide preliminary evidence for non-surgical interventions for AT, but lack key quality components as outlined in the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) Statement. The aim of this study was to conduct a systematic review and meta-analysis (where possible) of the evidence for physical therapies for AT management.
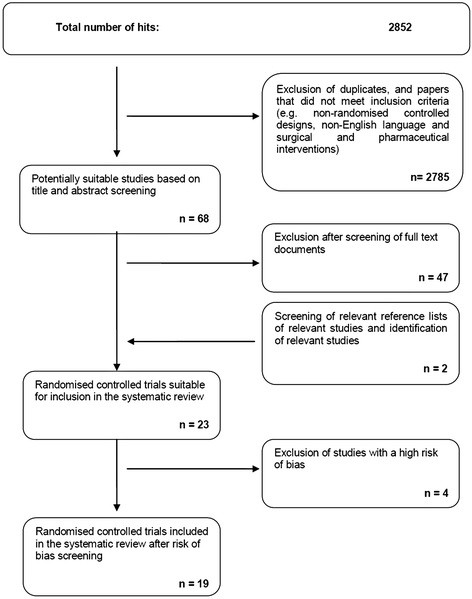
Methods: A comprehensive strategy was used to search 11 electronic databases from inception to September 2011. Search terms included Achilles, tendinopathy, pain, physical therapies, electrotherapy and exercise (English language full-text publications, human studies). Reference lists of eligible papers were hand-searched. Randomised controlled trials (RCTs) were included if they evaluated at least one non-pharmacological, non-surgical intervention for AT using at least one outcome of pain and/or function. Two independent reviewers screened 2852 search results, identifying 23 suitable studies, and assessed methodological quality and risk of bias using a modified PEDro scale. Effect size calculation and meta-analyses were based on fixed and random effects models respectively.
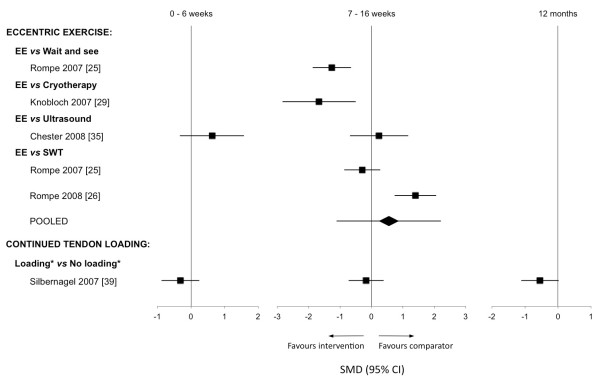
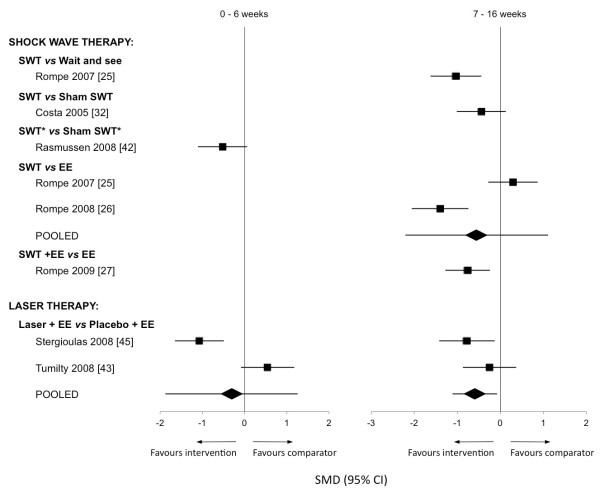
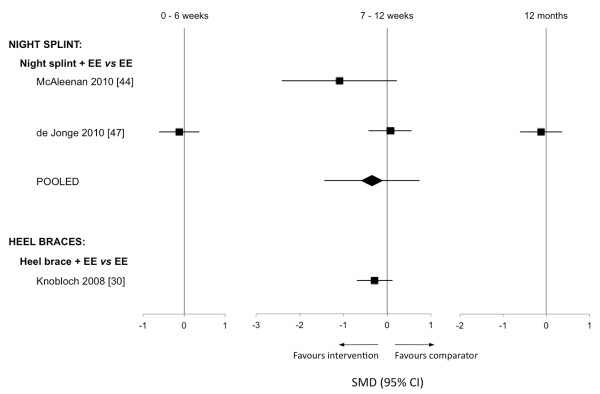
Results: Methodological quality ranged from 2 to 12 (/14). Four studies were excluded due to high risk of bias, leaving 19 studies, the majority of which evaluated midportion AT. Effect sizes from individual RCTs support the use of eccentric exercise. Meta-analyses identified significant effects favouring the addition of laser therapy to eccentric exercise at 12 weeks (pain VAS: standardised mean difference -0.59, 95% confidence interval -1.11 to -0.07), as well as no differences in effect between eccentric exercise and shock wave therapy at 16 weeks (VISA-A:-0.55,-2.21 to 1.11). Pooled data did not support the addition of night splints to eccentric exercise at 12 weeks (VISA-A:-0.35,-1.44 to 0.74). Limited evidence from an individual RCT suggests microcurrent therapy to be an effective intervention.
Conclusions: Practitioners can consider eccentric exercise as an initial intervention for AT, with the addition of laser therapy as appropriate. Shock wave therapy may represent an effective alternative. High-quality RCTs following CONSORT guidelines are required to further evaluate the efficacy of physical therapies and determine optimal clinical pathways for AT.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
