

Clusters of activated microglia in normal-appearing white matter show signs of innate immune activation
- PMID: 22747960
- PMCID: PMC3411485
- DOI: 10.1186/1742-2094-9-156
Clusters of activated microglia in normal-appearing white matter show signs of innate immune activation
Abstract
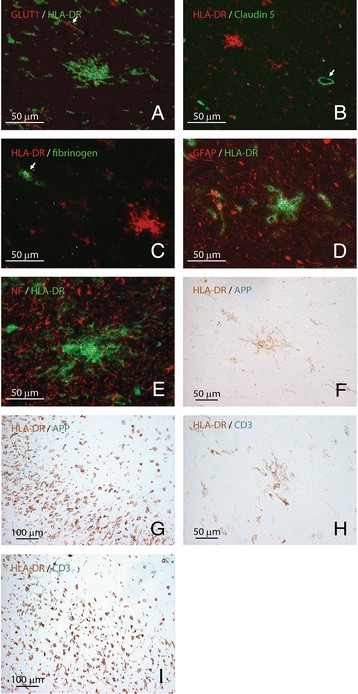
Background: In brain tissues from multiple sclerosis (MS) patients, clusters of activated HLA-DR-expressing microglia, also referred to as preactive lesions, are located throughout the normal-appearing white matter. The aim of this study was to gain more insight into the frequency, distribution and cellular architecture of preactive lesions using a large cohort of well-characterized MS brain samples.
Methods: Here, we document the frequency of preactive lesions and their association with distinct white matter lesions in a cohort of 21 MS patients. Immunohistochemistry was used to gain further insight into the cellular and molecular composition of preactive lesions.
Results: Preactive lesions were observed in a majority of MS patients (67%) irrespective of disease duration, gender or subtype of disease. Microglial clusters were predominantly observed in the vicinity of active demyelinating lesions and are not associated with T cell infiltrates, axonal alterations, activated astrocytes or blood-brain barrier disruption. Microglia in preactive lesions consistently express interleukin-10 and TNF-α, but not interleukin-4, whereas matrix metalloproteases-2 and -9 are virtually absent in microglial nodules. Interestingly, key subunits of the free-radical-generating enzyme NADPH oxidase-2 were abundantly expressed in microglial clusters.
Conclusions: The high frequency of preactive lesions suggests that it is unlikely that most of them will progress into full-blown demyelinating lesions. Preactive lesions are not associated with blood-brain barrier disruption, suggesting that an intrinsic trigger of innate immune activation, rather than extrinsic factors crossing a damaged blood-brain barrier, induces the formation of clusters of activated microglia.
Figures




References
-
- Bo L, Vedeler CA, Nyland HI, Trapp BD, Mørk SJ. Subpial demyelination in the cerebral cortex of multiple sclerosis patients. J Neuropathol Exp Neurol. 2003;62:723–732. - PubMed
-
- Barnett MH, Prineas JW. Relapsing and remitting multiple sclerosis: pathology of the newly forming lesion. Ann Neurol. 2004;5:458–468. - PubMed
-
- Hendriks JJ, Teunissen CE, de Vries HE, Dijkstra CD. Macrophages and neurodegeneration. Brain Res Brain Res Rev. 2005;48:185–195. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
