

'The influence of gestational age and socioeconomic status on neonatal outcomes in late preterm and early term gestation: a population based study'
- PMID: 22748037
- PMCID: PMC3464782
- DOI: 10.1186/1471-2393-12-62
'The influence of gestational age and socioeconomic status on neonatal outcomes in late preterm and early term gestation: a population based study'
Abstract
Background: Infants born late preterm (34 + 0 to 36 + 6 weeks GA (gestational age)) are known to have higher neonatal morbidity than term (37 + 0 to 41 + 6 weeks GA) infants. There is emerging evidence that these risks may not be homogenous within the term cohort and may be higher in early term (37 + 0 to 38 + 6 weeks GA). These risks may also be affected by socioeconomic status, a risk factor for preterm birth.
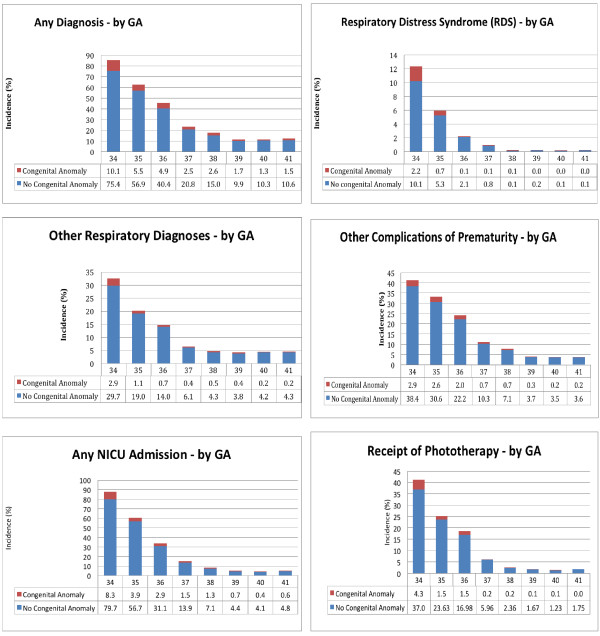
Methods: A retrospective population based cohort of infants born at 34 to 41 weeks of GA was assembled; individual and area-level income was used to develop three socioeconomic (SES) groups. Neonatal morbidity was grouped into respiratory distress syndrome (RDS), other respiratory disorders, other complications of prematurity, admission to a Level II/III nursery and receipt of phototherapy. Regression models were constructed to examine the relationship of GA and SES to neonatal morbidity while controlling for other perinatal variables.
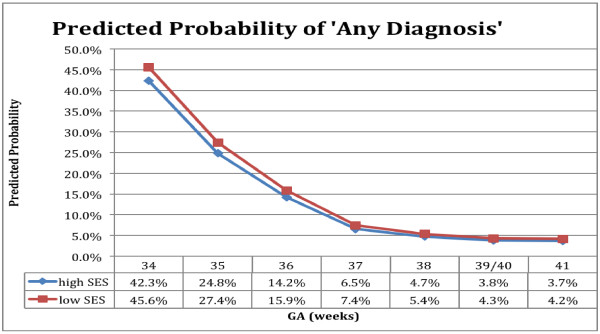
Results: The cohort contained 25 312 infants of whom 6.1% (n = 1524) were born preterm and 32.4% (n = 8203) were of low SES. Using 39/40 weeks GA as the reference group there was a decrease in neonatal morbidity at each week of gestation. The odds ratios remained significantly higher at 37 weeks for RDS or other respiratory disorders, and at 38 weeks for all other outcomes. SES had an independent effect, increasing morbidity with odds ratios ranging from 1.2-1.5 for all outcomes except for the RDS group, where it was not significant.
Conclusions: The risks of morbidity fell throughout late preterm and early term gestation for both respiratory and non-respiratory morbidity. Low SES was associated with an independent increased risk. Recognition that the morbidities associated with prematurity continue into early term gestation and are further compounded by SES is important to develop strategies for improving care of early term infants, avoiding iatrogenic complications and prioritizing public health interventions.
Figures
References
-
- Raju TNK. The problem of late-preterm (near-term) births: a workshop summary. Pediatr Res. 2006;60:775–776. - PubMed
-
- Gilbert WM, Nesbitt TS, Danielsen B. The cost of prematurity: quantification by gestational age and birth weight. Obstet Gynecol. 2003;102:488–492. - PubMed
-
- Martens PJ, Derksen S, Gupta S. Predictors of hospital readmission of Manitoba newborns within six weeks postbirth discharge: a population-based study. Pediatrics. 2004;114:708–713. - PubMed
-
- Escobar GJ, Clark RH, Greene JD. Short-term outcomes of infants born at 35 and 36 weeks gestation: we need to ask more questions. Semin Perinatol. 2006;30:28–33. - PubMed
-
- Escobar GJ, Joffe S, Gardner MN, Armstrong MA, Folck BF, Carpenter DM. Rehospitalization in the first two weeks after discharge from the neonatal intensive care unit. Pediatrics. 1999;104:e2. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
