

Persistence of complex vascular lesions despite prolonged prostacyclin therapy of pulmonary arterial hypertension
- PMID: 22748137
- PMCID: PMC4143476
- DOI: 10.1111/j.1365-2559.2012.04246.x
Persistence of complex vascular lesions despite prolonged prostacyclin therapy of pulmonary arterial hypertension
Abstract
Aims: Continuous infusion of prostacyclin analogues improves survival in advanced pulmonary arterial hypertension. In addition to its vasodilatory effects, prostacyclin has the potential to decrease inflammation, thrombosis, and smooth muscle proliferation. The aim of this retrospective study was to determine whether pathological data support the ability of prostanoids to prevent progression of vascular disease.
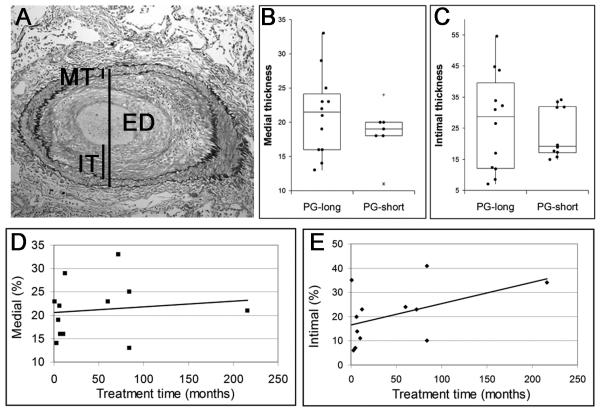
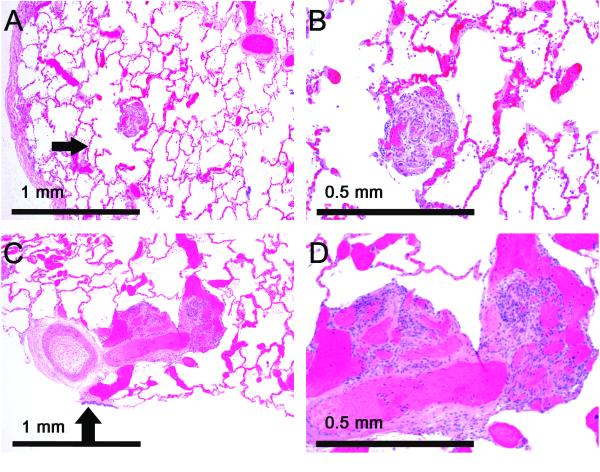
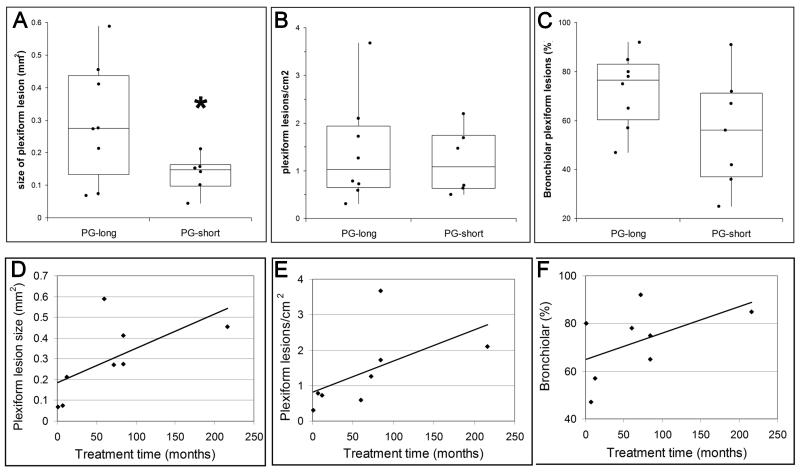
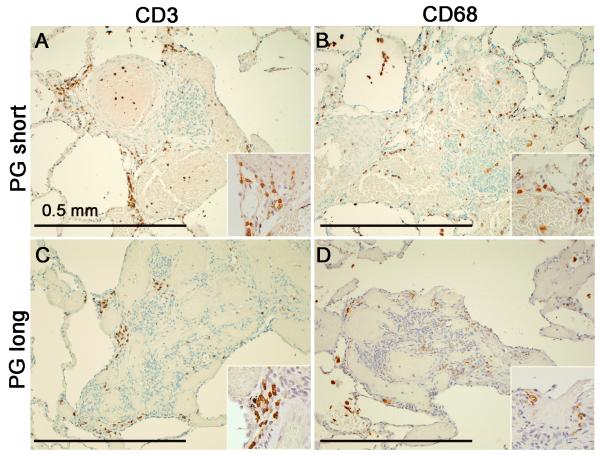
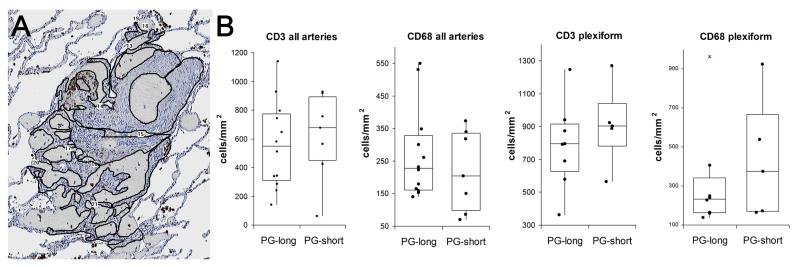
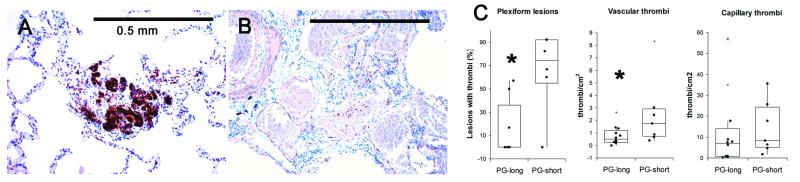
Methods and results: Twenty-two autopsied patients with World Health Organization category 1 pulmonary arterial hypertension (primarily idiopathic and connective tissue disease-associated) were divided into those who received long-term prostacyclin (n = 12, PG-long, mean treatment 3.9 years) and those who received 0-1 month of prostacyclin (n = 10, PG-short). Surprisingly, PG-long patients had larger plexiform lesions (P < 0.05), with no decrease in medial and intimal thicknesses as compared with PG-short patients. Plexiform lesion size and density increased with increasing treatment time. Also, PG-long patients had fewer platelet thrombi and more frequent acute diffuse alveolar haemorrhage. Quantification of macrophages and T cells revealed no differences in inflammatory infiltrates.
Conclusion: Although long-term prostacyclin therapy may have an antithrombotic effect in addition to its vasodilatory actions, it was not associated with the prevention of advanced vascular lesions. The mechanism by which prostacyclin analogues improve survival in pulmonary arterial hypertension remains uncertain.
Keywords: histopathology; plexiform lesions; prostaglandins; vascular remodelling.
© 2012 Blackwell Publishing Ltd.
Figures
References
-
- Stewart S, Rassl D. Advances in the understanding and classification of pulmonary hypertension. Histopathology. 2009;54:104–116. - PubMed
-
- Pietra GG, Capron F, Stewart S, et al. Pathologic assessment of vasculopathies in pulmonary hypertension. J. Am. Coll. Cardiol. 2004;43(12 Suppl. S):25S–32S. - PubMed
-
- Fuster V, Steele PM, Edwards WD, Gersh BJ, McGoon MD, Frye RL. Primary pulmonary hypertension: natural history and the importance of thrombosis. Circulation. 1984;70:580–587. - PubMed
-
- Barst RJ, Rubin LJ, Long WA, et al. A comparison of continuous intravenous epoprostenol (prostacyclin) with conventional therapy for primary pulmonary hypertension. The Primary Pulmonary Hypertension Study Group. N. Engl. J. Med. 1996;334:296–302. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
