

Long-term follow-up of the RTOG 9501/intergroup phase III trial: postoperative concurrent radiation therapy and chemotherapy in high-risk squamous cell carcinoma of the head and neck
- PMID: 22749632
- PMCID: PMC3465463
- DOI: 10.1016/j.ijrobp.2012.05.008
Long-term follow-up of the RTOG 9501/intergroup phase III trial: postoperative concurrent radiation therapy and chemotherapy in high-risk squamous cell carcinoma of the head and neck
Abstract
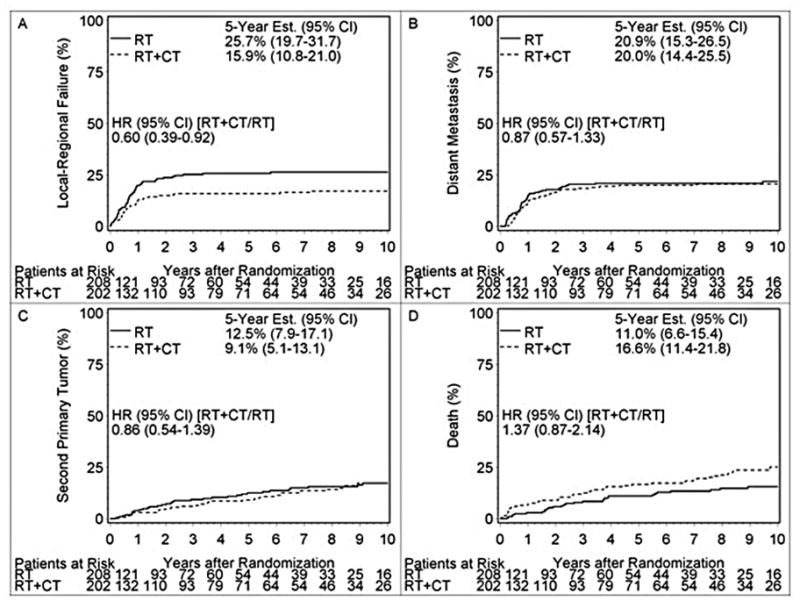
Purpose: Previous analysis of this Intergroup trial demonstrated that with a median follow-up among surviving patients of 45.9 months, the concurrent postoperative administration of cisplatin and radiation therapy improved local-regional control and disease-free survival of patients who had high-risk resectable head-and-neck carcinomas. With a minimum of 10 years of follow-up potentially now available for all patients, these results are updated here to examine long-term outcomes.
Methods and materials: A total of 410 analyzable patients who had high-risk resected head-and-neck cancers were prospectively randomized to receive either radiation therapy (RT: 60 Gy in 6 weeks) or identical RT plus cisplatin, 100 mg/m(2)i.v. on days 1, 22, and 43 (RT + CT).
Results: At 10 years, the local-regional failure rates were 28.8% vs 22.3% (P=.10), disease-free survival was 19.1% vs 20.1% (P=.25), and overall survival was 27.0% vs 29.1% (P=.31) for patients treated by RT vs RT + CT, respectively. In the unplanned subset analysis limited to patients who had microscopically involved resection margins and/or extracapsular spread of disease, local-regional failure occurred in 33.1% vs 21.0% (P=.02), disease-free survival was 12.3% vs 18.4% (P=.05), and overall survival was 19.6% vs 27.1% (P=.07), respectively.
Conclusion: At a median follow-up of 9.4 years for surviving patients, no significant differences in outcome were observed in the analysis of all randomized eligible patients. However, analysis of the subgroup of patients who had either microscopically involved resection margins and/or extracapsular spread of disease showed improved local-regional control and disease-free survival with concurrent administration of chemotherapy. The remaining subgroup of patients who were enrolled only because they had tumor in 2 or more lymph nodes did not benefit from the addition of CT to RT.
Trial registration: ClinicalTrials.gov NCT00002670.
Copyright © 2012 Elsevier Inc. All rights reserved.
Figures
References
-
- Cooper JS, Pajak TF, Forastierre A, et al. Precisely Defining High-Risk Operable Head and Neck Tumors Based on RTOG #85-03 and #88-24: Targets For PostOperative Radiochemotherapy. Head and Neck. 1998;20(7):588–594. - PubMed
-
- Morris M, Eifel PJ, Lu J, Grigsby PW, et al. Pelvic radiation with concurrent chemotherapy compared with pelvic and para-aortic radiation for high-risk cervical cancer. N Engl J Med. 1999 Apr 15;340(15):1137–43. - PubMed
-
- Cooper JS, Guo M, Herskovic A, et al. Chemoradiotherapy of Locally Advanced Esophageal Cancer: Long-term Follow-up of a Prospective Randomized Intergroup Trial (RTOG 85-01) JAMA. 1999;281:1623–27. - PubMed
-
- Al-Sarraf M, LeBlanc M, Shanker Giri PG, et al. Chemoradiotherapy Versus Radiotherapy in Patients With Advanced Nasopharyngeal Cancer: Phase III Randomized Intergroup Study 0099. J Clin Oncol. 1998;16:1310–1317. - PubMed
-
- Calais G, Alfonsi M, Bardet E, et al. Randomized Trial of Radiation Therapy Versus Concomitant Chemotherapy and Radiation Therapy for Advanced-Stage Oropharynx Carcinoma. J Natl Cancer Inst. 1999;91:2081–6. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
