

Protecting patients from an unsafe system: the etiology and recovery of intraoperative deviations in care
- PMID: 22750753
- PMCID: PMC3415974
- DOI: 10.1097/SLA.0b013e3182602564
Protecting patients from an unsafe system: the etiology and recovery of intraoperative deviations in care
Abstract
Objective: To understand the etiology and resolution of unanticipated events in the operating room (OR).
Background: The majority of surgical adverse events occur intraoperatively. The OR represents a complex, high-risk system. The influence of different human, team, and organizational/environmental factors on safety and performance is unknown.
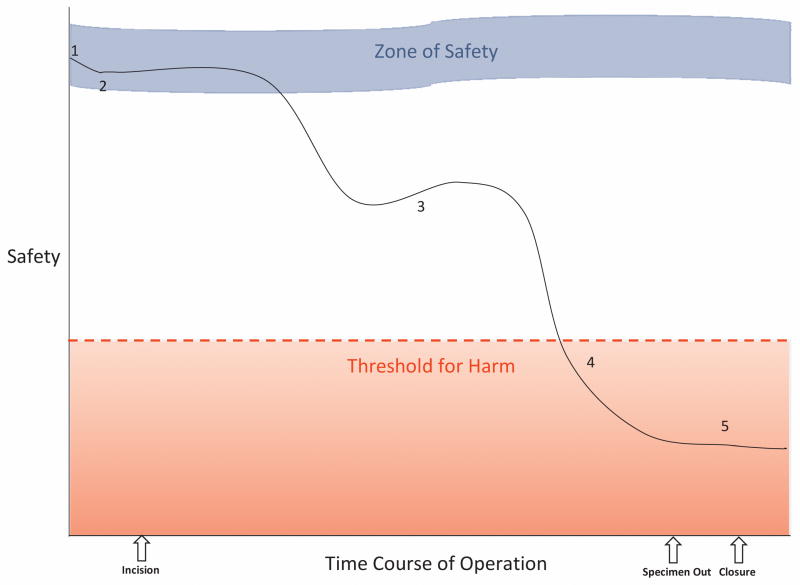
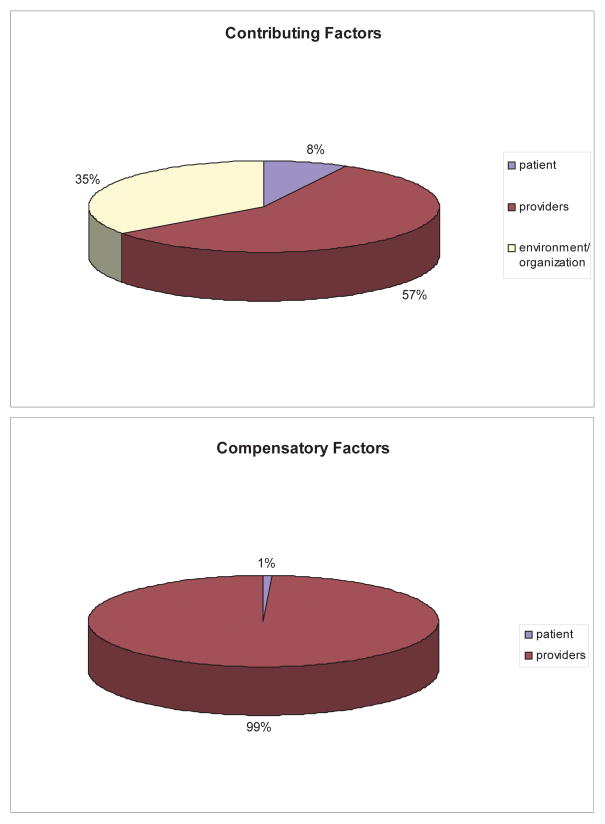
Methods: We video-recorded and transcribed 10 high-acuity operations, representing 43.7 hours of patient care. Deviations, defined as delays and/or episodes of decreased patient safety, were identified by majority consensus of a multidisciplinary team. Factors that contributed to each event and/or mitigated its impact were determined and attributed to the patient, providers, or environment/organization.
Results: Thirty-three deviations (10 delays, 17 safety compromises, 6 both) occurred--with a mean of 1 every 79.4 minutes. These deviations were multifactorial (mean 3.1 factors). Problems with communication and organizational structure appeared repeatedly at the root of both types of deviations. Delays tended to be resolved with vigilance, communication, coordination, and cooperation, while mediation of safety compromises was most frequently accomplished with vigilance, leadership, communication, and/or coordination. The organization/environment was not found to play a direct role in compensation.
Conclusions: Unanticipated events are common in the OR. Deviations result from poor organizational/environmental design and suboptimal team dynamics, with caregivers compensating to avoid patient harm. Although recognized in other high-risk domains, such human resilience has not yet been described in surgery and has major implications for the design of safety interventions.
Conflict of interest statement
Figures

Comment in
-
Celebrating human resilience to provide safe care.Ann Surg. 2012 Aug;256(2):211-2. doi: 10.1097/SLA.0b013e3182602565. Ann Surg. 2012. PMID: 22750754 No abstract available.
References
-
- [Accessed 28 April, 2011];What is Ergonomics? at http://www.iea.cc/01_what/What%20is%20Ergonomics.html.
-
- Carthey J, de Leval MR, Reason JT. The human factor in cardiac surgery: errors and near misses in a high technology medical domain. Ann Thorac Surg. 2001;72:300–5. - PubMed
-
- de Leval MR, Carthey J, Wright DJ, et al. Human factors and cardiac surgery: a multicenter study. J Thorac Cardiovasc Surg. 2000;119:661–72. - PubMed
-
- Mazzocco K, Petitti DB, Fong KT, et al. Surgical team behaviors and patient outcomes. Am J Surg. 2009;197:678–85. - PubMed
-
- Rogers SO, Jr, Gawande AA, Kwaan M, et al. Analysis of surgical errors in closed malpractice claims at 4 liability insurers. Surgery. 2006;140:25–33. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
