

Effect of a pharmacist intervention on clinically important medication errors after hospital discharge: a randomized trial
- PMID: 22751755
- PMCID: PMC3575734
- DOI: 10.7326/0003-4819-157-1-201207030-00003
Effect of a pharmacist intervention on clinically important medication errors after hospital discharge: a randomized trial
Abstract
Background: Clinically important medication errors are common after hospital discharge. They include preventable or ameliorable adverse drug events (ADEs), as well as medication discrepancies or nonadherence with high potential for future harm (potential ADEs).
Objective: To determine the effect of a tailored intervention on the occurrence of clinically important medication errors after hospital discharge.
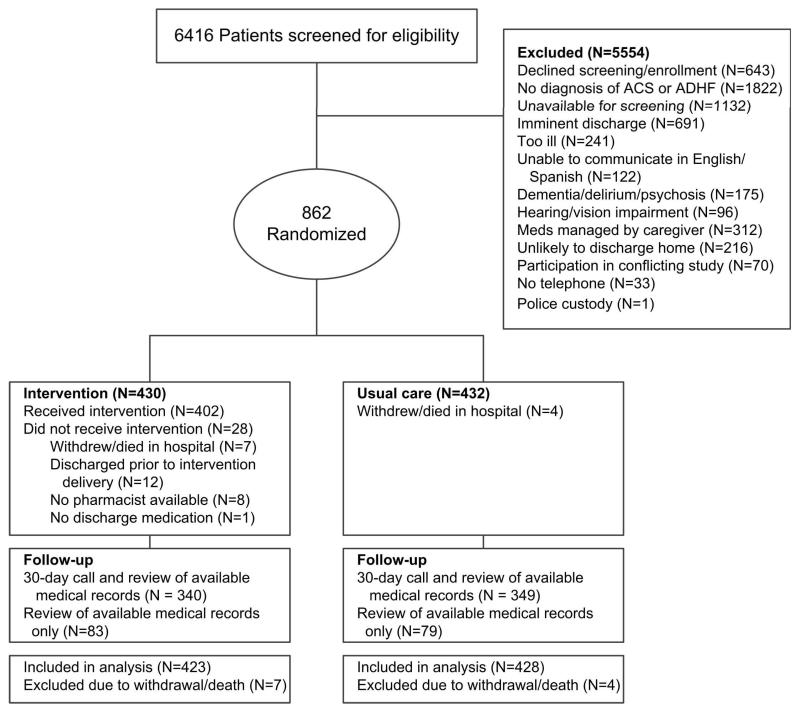
Design: Randomized, controlled trial with concealed allocation and blinded outcome assessors. (ClinicalTrials.gov registration number: NCT00632021)
Setting: Two tertiary care academic hospitals.
Patients: Adults hospitalized with acute coronary syndromes or acute decompensated heart failure.
Intervention: Pharmacist-assisted medication reconciliation, inpatient pharmacist counseling, low-literacy adherence aids, and individualized telephone follow-up after discharge.
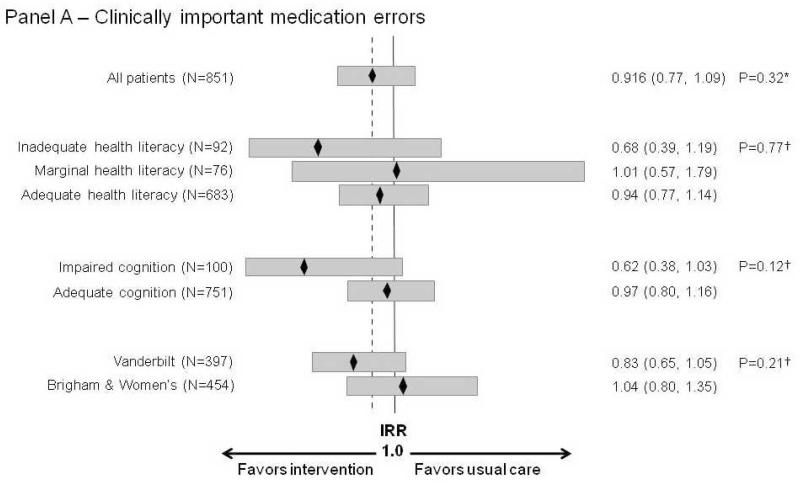
Measurements: The primary outcome was the number of clinically important medication errors per patient during the first 30 days after hospital discharge. Secondary outcomes included preventable or ameliorable ADEs, as well as potential ADEs.
Results: Among 851 participants, 432 (50.8%) had 1 or more clinically important medication errors; 22.9% of such errors were judged to be serious and 1.8% life-threatening. Adverse drug events occurred in 258 patients (30.3%) and potential ADEs in 253 patients (29.7%). The intervention did not significantly alter the per-patient number of clinically important medication errors (unadjusted incidence rate ratio, 0.92 [95% CI, 0.77 to 1.10]) or ADEs (unadjusted incidence rate ratio, 1.09 [CI, 0.86 to 1.39]). Patients in the intervention group tended to have fewer potential ADEs (unadjusted incidence rate ratio, 0.80 [CI, 0.61 to 1.04]).
Limitation: The characteristics of the study hospitals and participants may limit generalizability.
Conclusion: Clinically important medication errors were present among one half of patients after hospital discharge and were not significantly reduced by a health-literacy-sensitive, pharmacist-delivered intervention.
Primary funding source: National Heart, Lung, and Blood Institute.
Figures
Comment in
-
Effect of a pharmacist intervention.Ann Intern Med. 2013 Jan 15;158(2):137. doi: 10.7326/0003-4819-158-2-201301150-00013. Ann Intern Med. 2013. PMID: 23318317 No abstract available.
-
Effect of a pharmacist intervention.Ann Intern Med. 2013 Jan 15;158(2):137. doi: 10.7326/0003-4819-158-2-201301150-00014. Ann Intern Med. 2013. PMID: 23318318 No abstract available.
-
Effect of a pharmacist intervention.Ann Intern Med. 2013 Jan 15;158(2):137-8. doi: 10.7326/0003-4819-158-2-201301150-00015. Ann Intern Med. 2013. PMID: 23318319 No abstract available.
Summary for patients in
-
Summaries for patients. Medication errors after hospital discharge.Ann Intern Med. 2012 Jul 3;157(1):I-32. doi: 10.7326/0003-4819-157-1-201207030-00001. Ann Intern Med. 2012. PMID: 22751776 No abstract available.
References
-
- Kripalani S, Jackson AT, Schnipper JL, Coleman EA. Promoting effective transitions of care at hospital discharge: a review of key issues for hospitalists. Journal of Hospital Medicine. 2007;2(5):314–23. - PubMed
-
- Bates DW, Cullen DJ, Laird N, Petersen LA, Small SD, Servi D, et al. ADE Prevention Study Group Incidence of adverse drug events and potential adverse drug events. Implications for prevention. JAMA. 1995;274(1):29–34. - PubMed
-
- Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138:161–7. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical