

Ki-67 is a prognostic biomarker of survival after radiofrequency ablation of liver malignancies
- PMID: 22752375
- PMCID: PMC4122119
- DOI: 10.1245/s10434-012-2461-9
Ki-67 is a prognostic biomarker of survival after radiofrequency ablation of liver malignancies
Abstract
Purpose: To assess the predictive value of examinations of tissue adherent to multitined electrodes on local tumor progression-free survival (LPFS) and overall survival (OS) after liver tumor radiofrequency ablation (RFA).
Methods: An institutional review board-approved, Health Insurance Portability and Accountability Act-compliant review identified 68 liver tumors treated with RFA in 63 patients with at least 3 years' follow-up. Tissue adherent to the electrode after liver tumor RFA was evaluated with proliferation (Ki-67) and apoptotic (caspase-3) markers. LPFS and OS were evaluated by Kaplan-Meier methodology and the log-rank test. Multivariate analysis assessed the effect of tumor size, pathology, and post-RFA tissue characteristics on LPFS and OS.
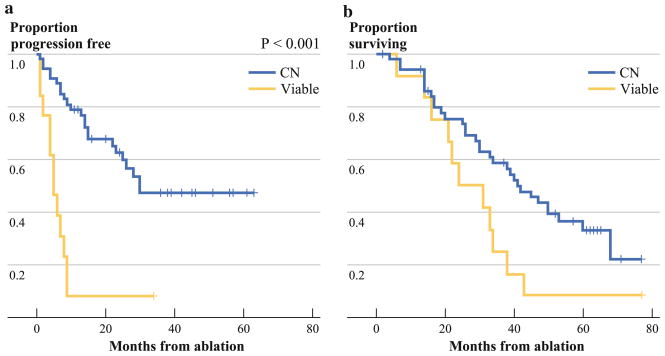
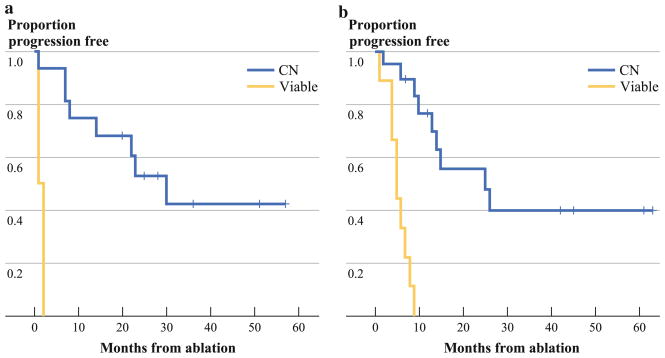
Results: Post-RFA tissue examination classified 55 of the 68 tumors as completely ablated with coagulation necrosis, with cells positive for caspase-3 and negative for Ki-67 (CN). Thirteen had viable Ki-67-positive tumor cells. Mean liver tumor size was larger in the viable (V) group versus the CN group (3.4 vs. 2.5 cm, respectively; P = .017). For the V and CN groups, respectively, local tumor progression occurred in 12 (92 %) of 13 and 23 (42 %) of 55 specimens. One, 3-, and 5-year LPFS was 8 %, 8 %, and 8 %, and 79 %, 47 %, and 47 % (P < .001) for the V and CN groups, respectively. During a 63-month median follow-up, 92 % of patients in the V group and 58 % in the CN group died, resulting in 1-, 3-, and 5-year OS of 92 %, 25 %, and 8 % vs. 92 %, 59 %, and 33 % (P = .032), respectively.
Conclusions: Ki-67-positive tumor cells on the electrode after liver tumor RFA is an independent predictor of LPFS and OS. Size, initially thought to be an independent risk factor for local tumor progression in tumors 3-5 cm, does not hold its significance at long follow-up.
Figures
References
-
- Motola-Kuba D, Zamora-Valdes D, Uribe M, Mendez-Sanchez N. Hepatocellular carcinoma. An overview. Ann Hepatol. 2006;5:16–24. - PubMed
-
- Hildebrand P, Kleemann M, Roblick UJ, et al. Radiofrequency-ablation of unresectable primary and secondary liver tumors: results in 88 patients. Langenbecks Arch Surg. 2006;391:1–6. - PubMed
-
- Hanna NN. Radiofrequency ablation of primary and metastatic hepatic malignancies. Clin Colorectal Cancer. 2004;4:92–100. - PubMed
-
- Curley SA, Izzo F. Radiofrequency ablation of primary and metastic liver tumors. Surg Technol Int. 2002;10:99–106. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
