

Prospective assessment of fetal-maternal cell transfer in miscarriage and pregnancy termination
- PMID: 22752611
- PMCID: PMC3415291
- DOI: 10.1093/humrep/des244
Prospective assessment of fetal-maternal cell transfer in miscarriage and pregnancy termination
Abstract
Background: Fetal cells (microchimerism) are acquired by women during pregnancy. Fetal microchimerism persists decades later and includes cells with pluripotent capacity. Persistent microchimerism has the capacity for both beneficial and detrimental maternal health consequences. Both miscarriage and termination of pregnancy can result in fetal microchimerism. We sought to determine whether cellular fetal microchimerism is acquired during management of pregnancy loss and further explored factors that could influence fetal cell transfer, including viability of fetal tissue, surgical versus medical management and gestational age.
Methods: Pregnant women (n= 150 samples from 75 women) with singleton pregnancies undergoing a TOP (n= 63) or treatment for embryonic or fetal demise (miscarriage, n= 12) were enrolled. Mononuclear cells were isolated from blood samples drawn before, and 30 min after, treatment. Fetal cellular microchimerism concentrations were determined using quantitative PCR for a Y chromosome-specific sequence, expressed as genome equivalents of fetal DNA per 100 000 maternal cell equivalents (gEq/10(5)). Detection rate ratios were determined according to clinical characteristics.
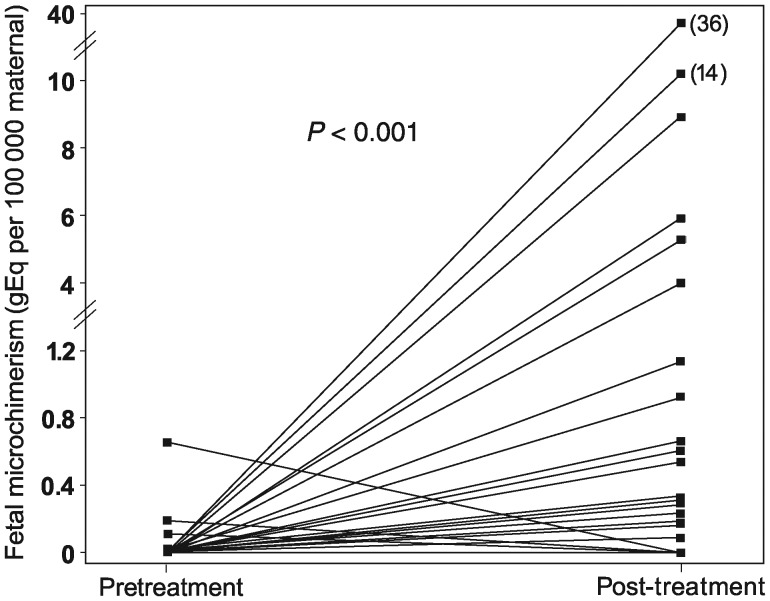
Results: Cellular fetal microchimerism was found more often in post- compared with pretreatment samples, 24 versus 5% (P= 0.004) and at higher concentrations, 0-36 versus 0-0.7 gEq/10(5) (P< 0.001). Likelihood of microchimerism was higher in surgical than medical management, detection rate ratio 24.7 (P= 0.02). The detection rate ratio for TOP versus miscarriage was 16.7 for known male fetuses (P= 0.02). Microchimerism did not vary with gestational age.
Conclusions: Significant fetal cell transfer occurs during miscarriage and TOP. Exploratory analyses support relationships between obstetric clinical factors and acquisition of fetal cellular microchimerism; however, our limited sample size precludes definitive analysis of these relationships, and confirmation is needed. In addition, the long-term persistence and potential consequences of fetal microchimerism on maternal health merit further investigation.
Figures
Similar articles
-
Fetal cellular microchimerism in miscarriage and pregnancy termination.Chimerism. 2013 Oct-Dec;4(4):136-8. doi: 10.4161/chim.24915. Epub 2013 May 3. Chimerism. 2013. PMID: 23723084 Free PMC article.
-
Cellular fetal microchimerism in preeclampsia.Hypertension. 2013 Dec;62(6):1062-7. doi: 10.1161/HYPERTENSIONAHA.113.01486. Epub 2013 Oct 7. Hypertension. 2013. PMID: 24101661 Free PMC article.
-
Microchimerism in recurrent miscarriage.Cell Mol Immunol. 2014 Nov;11(6):589-94. doi: 10.1038/cmi.2014.82. Epub 2014 Sep 22. Cell Mol Immunol. 2014. PMID: 25242272 Free PMC article.
-
Naturally acquired microchimerism.Int J Dev Biol. 2010;54(2-3):531-43. doi: 10.1387/ijdb.082767hg. Int J Dev Biol. 2010. PMID: 19924635 Free PMC article. Review.
-
Microchimerism in women with recurrent miscarriage.Chimerism. 2014;5(3-4):103-5. doi: 10.1080/19381956.2015.1017241. Epub 2015 Mar 16. Chimerism. 2014. PMID: 25779348 Free PMC article. Review.
Cited by
-
Fetal microchimerism by mode of delivery: a prospective cohort study.BJOG. 2019 Jan;126(1):24-31. doi: 10.1111/1471-0528.15432. Epub 2018 Sep 24. BJOG. 2019. PMID: 30102819 Free PMC article.
-
Lack of Evidence That Male Fetal Microchimerism is Present in Endometriosis.Reprod Sci. 2015 Sep;22(9):1115-21. doi: 10.1177/1933719115574343. Epub 2015 Mar 5. Reprod Sci. 2015. PMID: 25749809 Free PMC article.
-
Complex chimerism: pregnancy after solid organ transplantation.Chimerism. 2013 Jul-Sep;4(3):71-7. doi: 10.4161/chim.25401. Epub 2013 Jun 25. Chimerism. 2013. PMID: 23974274 Free PMC article.
-
Birth Order and Family Size of UK Biobank Subjects Identified as Asexual, Bisexual, Heterosexual, or Homosexual According to Self-Reported Sexual Histories.Arch Sex Behav. 2025 Jan;54(1):35-50. doi: 10.1007/s10508-024-03004-2. Epub 2024 Oct 1. Arch Sex Behav. 2025. PMID: 39354277 Free PMC article.
-
Genomic evidence of Y chromosome microchimerism in the endometrium during endometriosis and in cases of infertility.Reprod Biol Endocrinol. 2019 Feb 13;17(1):22. doi: 10.1186/s12958-019-0465-z. Reprod Biol Endocrinol. 2019. PMID: 30760267 Free PMC article.
References
-
- Ariga H, Ohto H, Busch MP, Imamura S, Watson R, Reed W, Lee T. Kinetics of fetal cellular and cell-free DNA in the maternal circulation during and after pregnancy: implications for noninvasive prenatal diagnosis. Transfusion. 2001;41:1524–1530. - PubMed
-
- Bianchi D, Farina A, Weber W, Delli-Bovi L, DeRiso M, Williams J, Klinger K. Significant fetal–maternal hemorrhage after termination of pregnancy: implications for development of fetal cell microchimerism. Am J Obstet Gynecol. 2001;184:703–706. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
