

A clinical decision aid for the selection of antithrombotic therapy for the prevention of stroke due to atrial fibrillation
- PMID: 22752615
- PMCID: PMC3432235
- DOI: 10.1093/eurheartj/ehs167
A clinical decision aid for the selection of antithrombotic therapy for the prevention of stroke due to atrial fibrillation
Abstract
Aims: The availability of new antithrombotic agents, each with a unique efficacy and bleeding profile, has introduced a considerable amount of clinical uncertainty with physicians. We have developed a clinical decision aid in order to assist clinicians in determining an optimal antithrombotic regime for the prevention of stroke in patients who are newly diagnosed with non-valvular atrial fibrillation.
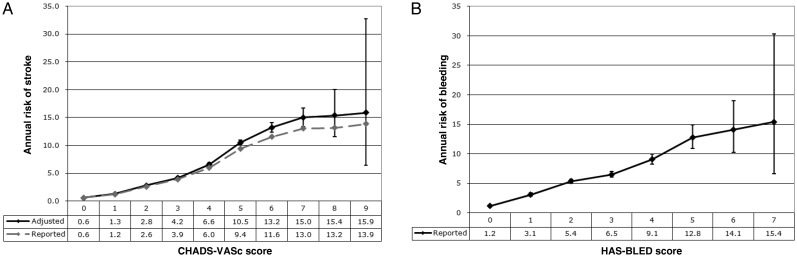
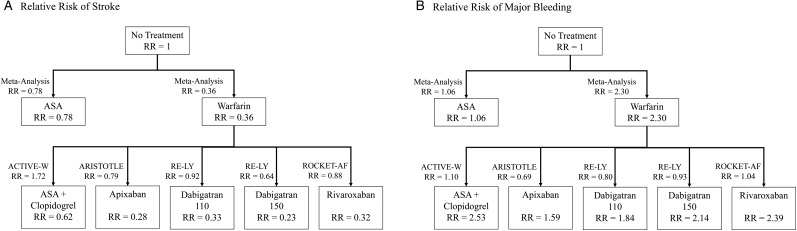
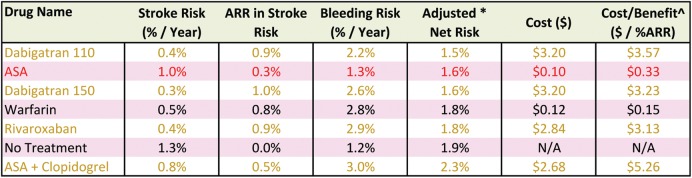
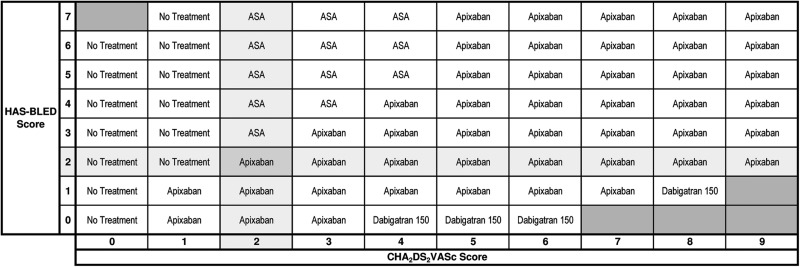
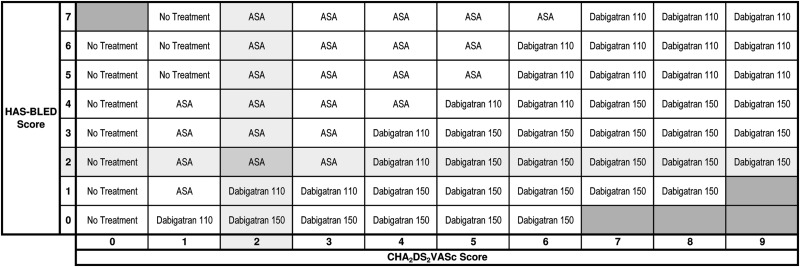
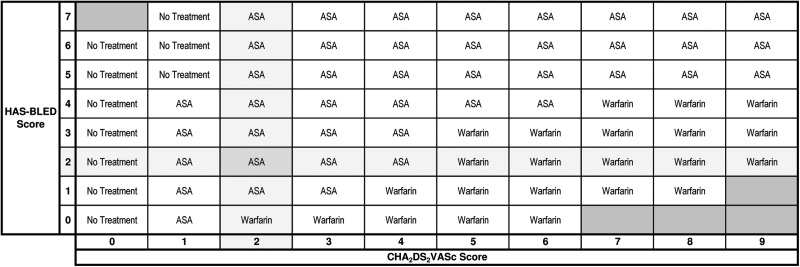
Methods and results: The CHA(2)DS(2)-VASc and HAS-BLED scoring systems were used to assess patients' baseline risks of stroke and major bleeding, respectively. The relative risks of stroke and major bleeding for each antithrombotic agent were then used to identify the agent associated with the lowest net risk. Individual patient factors such as the treatment threshold, bleeding ratio, and cost threshold modified the recommendations in order to generate a final recommendation. By considering both patient factors and clinical research concurrently, this clinical decision aid is able to provide specific advice to clinicians regarding an optimal stroke prevention strategy. The resulting treatment recommendation tables are consistent with the recommendations of the European Society of Cardiology and Canadian Cardiovascular Society Guidelines, which can be incorporated into either a paper-based or electronic format to allow clinicians to have decision support at the point of care.
Conclusion: The use of a clinical decision aid that considers both patient factors and evidence-based medicine will serve to bridge the knowledge gap and provide practical guidance to clinicians in the prevention of stroke due to atrial fibrillation.
Figures
References
-
- Fuster V, Rydén LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, Halperin JL, LeHeuzey J-Y, Kay GN, Lowe JE, Olsson SB, Prystowsky EN, Tamargo JL, Wann S. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation. Circulation. 2006;114:e257–e354. - PubMed
-
- Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med. 2007;146:857–867. - PubMed
-
- Connolly SJ, Ezekowitz MD, Yusuf S, Eikelboom J, Oldgren J, Parekh A, Pogue J, Reilly PA, Themeles E, Varrone J, Wang S, Alings M, Xavier D, Zhu J, Diaz R, Lewis BS, Darius H, Diener HC, Joyner CD, Wallentin L RE-LY Steering Committee and Investigators. Dabigatran versus Warfarin in Patients with Atrial Fibrillation. N Engl J Med. 2009;361:1139–1151. - PubMed
-
- Granger CB, Alexander JH, McMurray JJV, Lopes RD, Hylek EM, Hanna M, Al-Khalidi HR, Ansell J, Atar D, Avezum A, Bahit MC, Diaz R, Easton JD, Ezekowitz JA, Flaker G, Garcia D, Geraldes M, Gersh BJ, Golitsyn S, Goto S, Hermosillo AG, Hohnloser SH, Horowitz J, Mohan P, Jansky P, Lewis BS, Lopez-Sendon JL, Pais P, Parkhomenko A, Verheugt FWA, Zhu J, Wallentin L. Apixaban versus warfarin in patients with atrial fibrillation. N Eng J Med. 2011;365:981–992. - PubMed
-
- Patel MR, Mahaffey KW, Garg J, Pan G, Singer DE, Hacke W, Breithardt G, Halperin JL, Hankey GJ, Piccini JP, Becker RC, Nessel CC, Paolini JF, Berkowitz SD, Fox KAA, Califf RM the ROCKET AF Sterring Committee. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Eng J Med. 2011;365:883–891. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
