

Midtrimester amniotic fluid concentrations of interleukin-6 and interferon-gamma-inducible protein-10: evidence for heterogeneity of intra-amniotic inflammation and associations with spontaneous early (<32 weeks) and late (>32 weeks) preterm delivery
- PMID: 22752762
- PMCID: PMC3498502
- DOI: 10.1515/jpm-2012-0034
Midtrimester amniotic fluid concentrations of interleukin-6 and interferon-gamma-inducible protein-10: evidence for heterogeneity of intra-amniotic inflammation and associations with spontaneous early (<32 weeks) and late (>32 weeks) preterm delivery
Abstract
Introduction: Intra-amniotic inflammation is traditionally defined as an elevation of amniotic fluid interleukin (IL)-6. Previous case control studies have suggested an association between an elevated midtrimester amniotic fluid IL-6 and preterm delivery, although such an association has been recently challenged. Intra-amniotic inflammation can also be defined by an elevation of the T-cell chemokine, Interferon-gamma-inducible protein (IP)-10. An elevation in amniotic fluid IP-10 has been associated with chronic chorioamnionitis, a lesion frequently found in late spontaneous preterm birth and fetal death. In contrast, an elevation in amniotic fluid IL-6 is typically associated with acute chorioamnionitis and funisitis. This study was conducted to examine the relationship between an elevation in amniotic fluid IL-6 in the midtrimester and preterm delivery at or before 32 weeks of gestation, and the amniotic fluid concentration of IP-10 and preterm delivery after 32 weeks of gestation.
Materials and methods: This cohort study included 847 consecutive women undergoing genetic midtrimester amniocentesis; in 796 cases, amniotic fluid and pregnancy outcome was available for study after exclusion of abnormal karyotype and/or fetal congenital anomalies. Spontaneous preterm delivery was defined as early (≤32 weeks) or late (after 32 completed weeks of pregnancy). The amniotic fluid and maternal blood concentrations of IL-6 and IP-10 were measured by specific immunoassays.
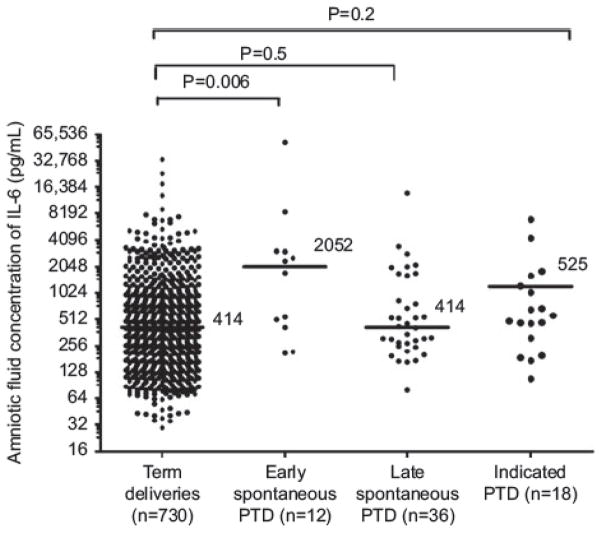
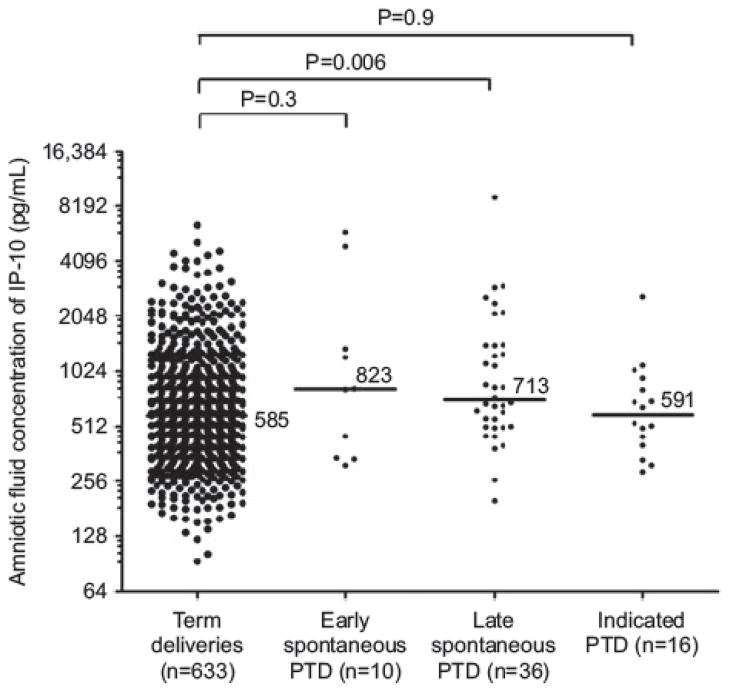
Results: 1) The prevalence of preterm delivery was 8.3% (66/796), while those of early and late spontaneous preterm delivery were 1.5% (n=12), and 4.5% (n=36), respectively; 2) patients who had a spontaneous preterm delivery after 32 weeks of gestation had a higher median amniotic fluid IP-10 concentration than those who delivered at term [median 713 pg/mL, inter-quartile range (IQR) 509-1427 pg/mL vs. median 589 pg/mL, IQR 402-953 pg/mL; P=0.006] and an elevation of amniotic fluid IP-10 concentration above 502 pg/mL (derived from an ROC curve) was associated with late spontaneous preterm delivery [odds ratio 3.9 (95% CI 1.6-9.9)]; 3) patients who had a spontaneous preterm delivery ≤32 weeks of gestation had a higher median amniotic fluid IL-6 concentration than those who delivered at term [median 2052 pg/mL, IQR 435-3015 pg/mL vs. median 414 pg/mL, IQR 209-930 pg/mL; P=0.006], and an elevated amniotic fluid IL-6 concentration above 1740 pg/mL (derived from an ROC curve) was associated with early spontaneous preterm delivery [odds ratio 9.5 (95% CI 2.9-31.1)]; 4) subclinical intra-amniotic inflammation, defined as an elevation of IL-6 (≥2.9 ng/mL) or IP-10 (≥2.2 ng/mL) concentration above the 95th percentile of patients who had uncomplicated term delivery (n=652 for IL-6 and n=633 for IP-10), was observed in 6.3% (50/796) and 5.8% (45/770) of cases, respectively. Although each type of inflammation is a risk factor for spontaneous preterm delivery, many patients had a term delivery without complication; 5) the amniotic fluid in the midtrimester did not contain microorganisms detectable with cultivation techniques.
Conclusions: INTRA-amniotic inflammation is heterogeneous. Some patients have elevated amniotic fluid concentrations of IL-6, and are at risk for spontaneous preterm delivery before 32 weeks of gestation, while others have an elevated IP-10 (a chemotactic T-cell chemokine) and such patients are at risk for spontaneous preterm delivery after 32 weeks of gestation. A fraction of patients have subclinical intra-amniotic inflammation and deliver at term. The clinical significance of this condition remains to be determined.
Figures
References
-
- Alanen A. Polymerase chain reaction in the detection of microbes in amniotic fluid. Ann Med. 1998;30:288– 95. - PubMed
-
- Andrews WW, Hauth JC, Goldenberg RL, Gomez R, Romero R, Cassell GH. Amniotic fluid interleukin-6: correlation with upper genital tract microbial colonization and gestational age in women delivered after spontaneous labor versus indicated delivery. Am J Obstet Gynecol. 1995;173:606– 12. - PubMed
-
- Apuzzio J, Chan Y, Al-Khan A, Illsley N, Kim PL, Vonhaggen S. Second-trimester amniotic fluid interleukin-10 concentration predicts preterm delivery. J Matern Fetal Neonatal Med. 2004;15:313– 7. - PubMed
-
- Arechavaleta-Velasco F, Koi H, Strauss JF, III, Parry S. Viral infection of the trophoblast: time to take a serious look at its role in abnormal implantation and placentation? J Reprod Immunol. 2002;55:113– 21. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources