

Relapse versus reinfection: recurrent Clostridium difficile infection following treatment with fidaxomicin or vancomycin
- PMID: 22752857
- PMCID: PMC3388025
- DOI: 10.1093/cid/cis357
Relapse versus reinfection: recurrent Clostridium difficile infection following treatment with fidaxomicin or vancomycin
Abstract
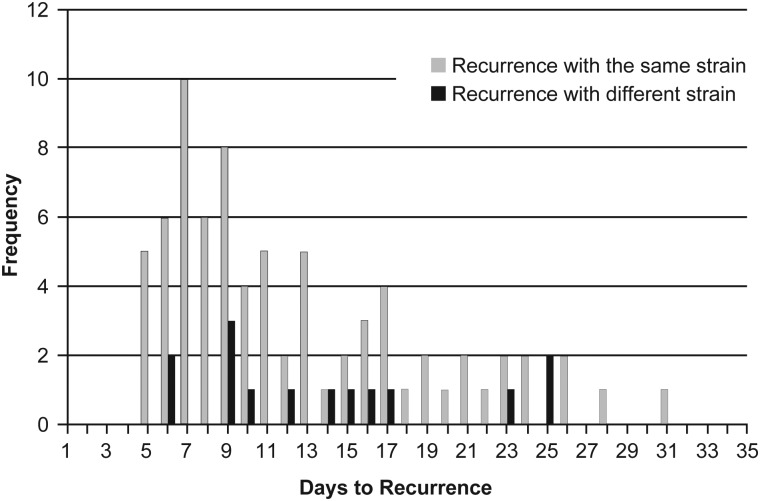
Our study sought to compare the strain types of Clostridium difficile causing initial and recurrent episodes of C. difficile infection (CDI) in adult patients with a first episode of CDI or 1 prior episode of CDI within the previous 90 days. Strains originated from patients who had been entered into two phase 3 randomized clinical trials of fidaxomicin versus vancomycin. Isolates of C. difficile from the initial and recurrent episodes within 28 (± 2) days of cure of CDI were compared using restriction endonuclease analysis (REA) typing. Paired isolates were available from 90 of 194 (46%) patients with recurrent CDI. Patients with isolates available were significantly younger (P = .008) and more likely to be from Canadian sites (P = .0001), compared with patients without isolates. In 75 of 90 subjects (83.3%), the identical REA type strain was identified at recurrence and the initial episode (putative relapse). Early recurrences (0-14 days after treatment completion) were relapses in 86.7% and a new strain (reinfection) in 13.3%. Later recurrences (15-31 days after treatment) were relapses in 76.7% and reinfections in 23.3%. Mean time (± standard deviation) to recurrence was 12.2 (± 6.4) days for relapses and 14.7 (± 6.8) days for reinfections (P = .177). The most common BI/NAP1/027 group and the previous US epidemic REA group J/NAP2/001 had a significantly higher combined rate of recurrence with the same strain (relapse), compared with the other REA groups (39 of 42 [93%] vs 36 of 48 [75%], respectively; P = .023). We found a higher than historic rate of recurrent CDI caused by the same isolate as the original episode, a finding that may be related to the relatively short observation period in this study and the high frequency of isolation of epidemic strains, such as groups BI and J, for which relapse rates may be higher than for other REA groups. Caution in generalizing these observations is required, because the patients studied were younger and more likely to be from Canadian sites than were patients with recurrence who did not provide isolates.
Trial registration: ClinicalTrials.gov NCT00314951 NCT00468728.
Figures
References
-
- Johnson S. Recurrent Clostridium difficile infection: a review of risk factors, treatments, and outcomes. J Infect. 2009;58:403–10. - PubMed
-
- Pepin J, Alary ME, Valiquette L. Increasing risk of relapse after treatment of Clostridium difficile colitis in Quebec, Canada. Clin Infect Dis. 2005;40:1591–7. - PubMed
-
- Johnson S, Adelmann A, Clabots CR, Peterson LR, Gerding DN. Recurrences of Clostridium difficile diarrhea not caused by the original infecting organism. J Infect Dis. 1989;159:340–3. - PubMed
-
- Wilcox MH, Fawley WN, Settle CD, Davidson A. Recurrence of symptoms in Clostridium difficile infection—relapse or reinfection? J Hosp Infect. 1998;38:93–100. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
