

Fidaxomicin versus vancomycin for Clostridium difficile infection: meta-analysis of pivotal randomized controlled trials
- PMID: 22752871
- PMCID: PMC3388031
- DOI: 10.1093/cid/cis499
Fidaxomicin versus vancomycin for Clostridium difficile infection: meta-analysis of pivotal randomized controlled trials
Abstract
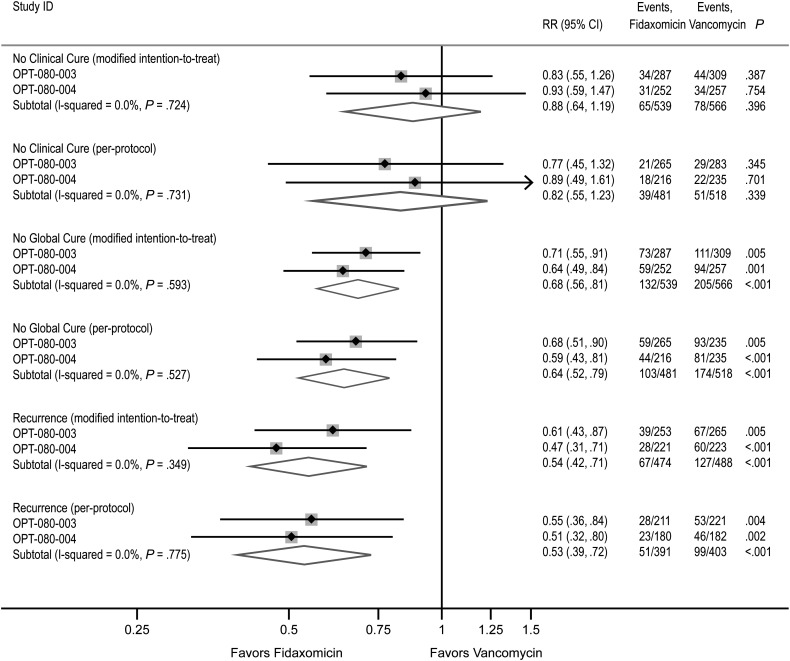
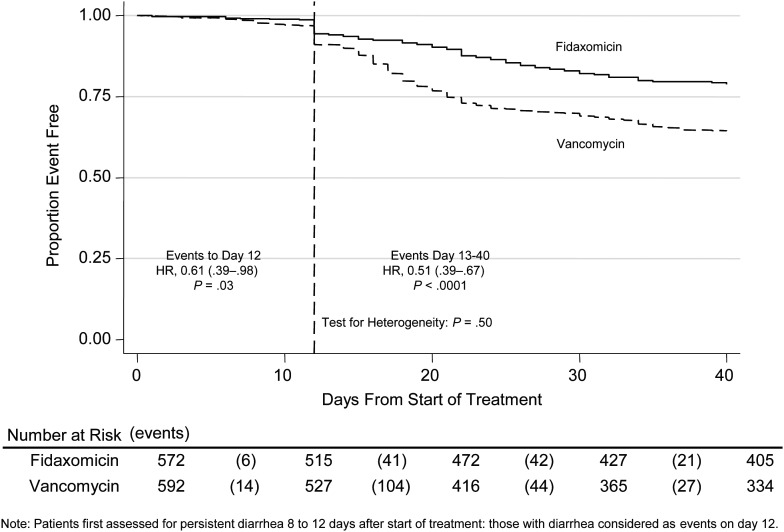
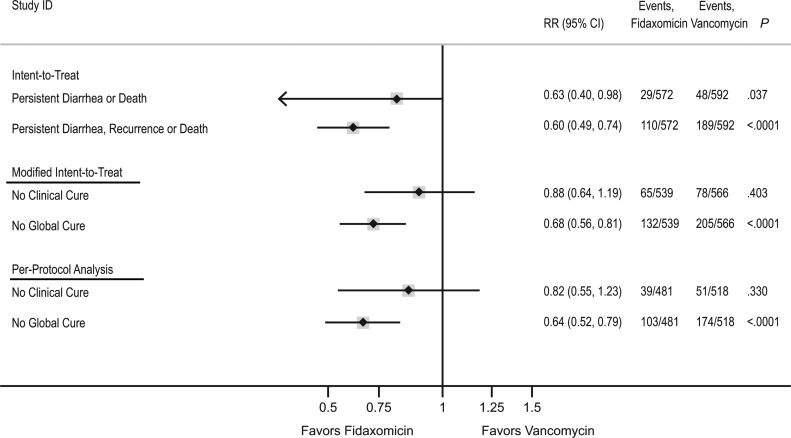
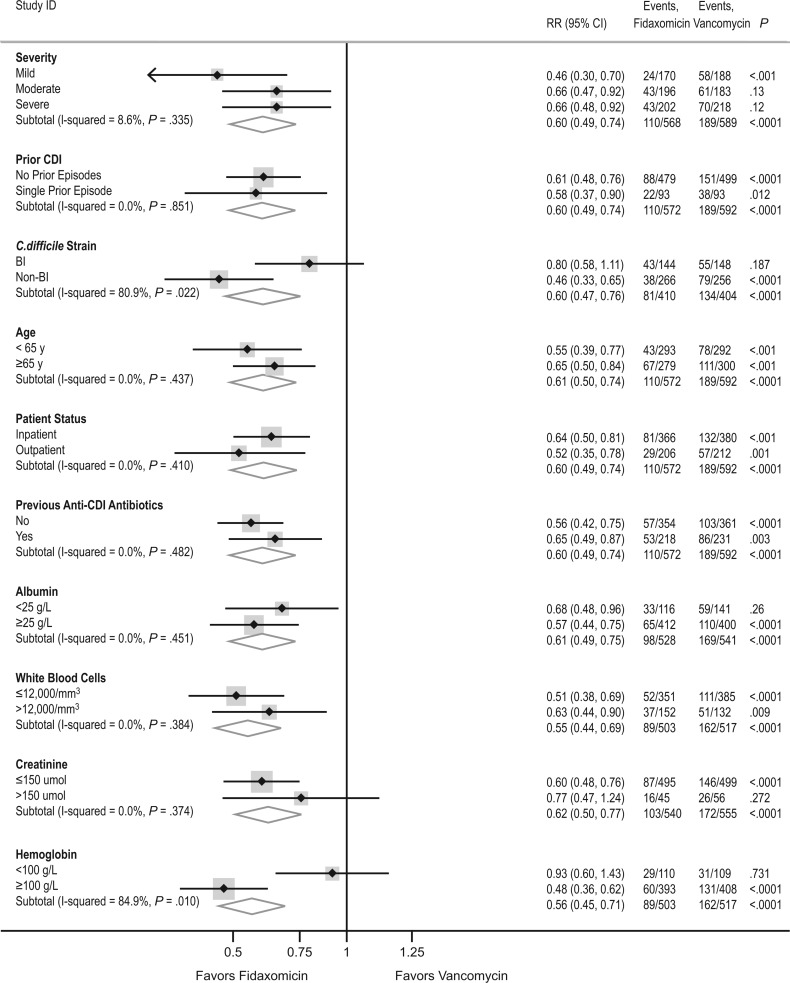
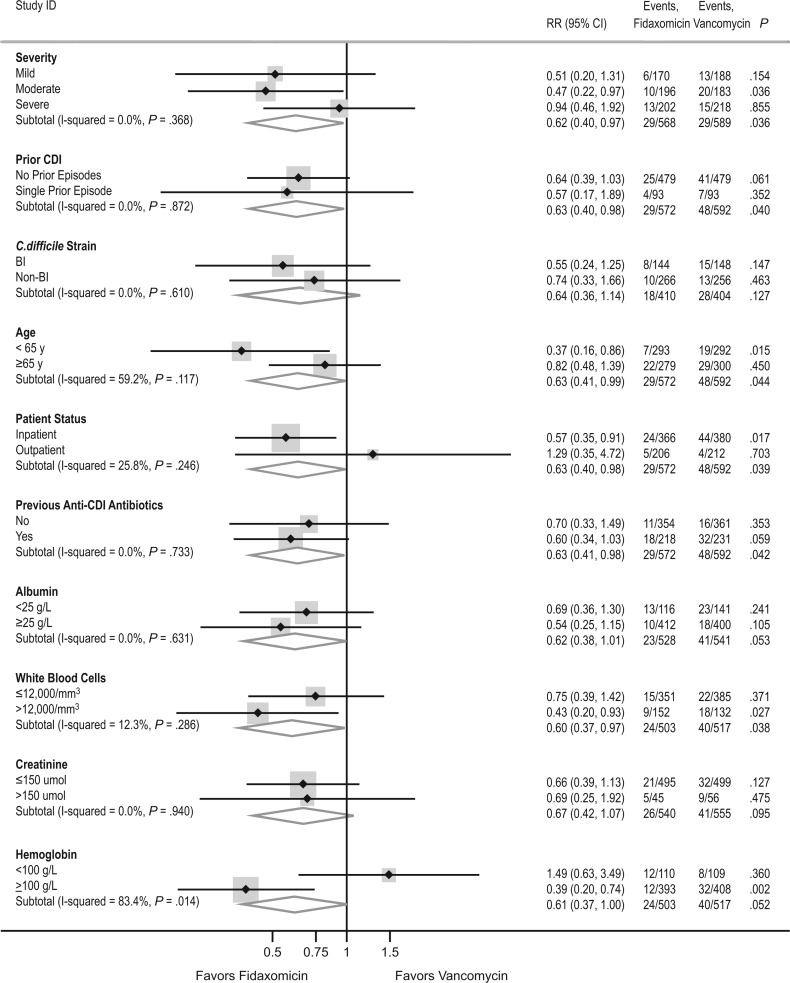
Two recently completed phase 3 trials (003 and 004) showed fidaxomicin to be noninferior to vancomycin for curing Clostridium difficile infection (CDI) and superior for reducing CDI recurrences. In both studies, adults with active CDI were randomized to receive blinded fidaxomicin 200 mg twice daily or vancomycin 125 mg 4 times a day for 10 days. Post hoc exploratory intent-to-treat (ITT) time-to-event analyses were undertaken on the combined study 003 and 004 data, using fixed-effects meta-analysis and Cox regression models. ITT analysis of the combined 003/004 data for 1164 patients showed that fidaxomicin reduced persistent diarrhea, recurrence, or death by 40% (95% confidence interval [CI], 26%-51%; P < .0001) compared with vancomycin through day 40. A 37% (95% CI, 2%-60%; P = .037) reduction in persistent diarrhea or death was evident through day 12 (heterogeneity P = .50 vs 13-40 days), driven by 7 (1.2%) fidaxomicin versus 17 (2.9%) vancomycin deaths at <12 days. Low albumin level, low eosinophil count, and CDI treatment preenrollment were risk factors for persistent diarrhea or death at 12 days, and CDI in the previous 3 months was a risk factor for recurrence (all P < .01). Fidaxomicin has the potential to substantially improve outcomes from CDI.
Figures
References
-
- McDonald LC, Killgore GE, Thompson A, et al. An epidemic, toxin gene-variant strain of Clostridium difficile. N Engl J Med. 2005;353:2433–41. - PubMed
-
- Loo VG, Poirier L, Miller MA, et al. A predominantly clonal multi-institutional outbreak of Clostridium difficile-associated diarrhea with high morbidity and mortality. N Engl J Med. 2005;353:2442–9. - PubMed
-
- Muto CA, Pokrywka M, Shutt K, et al. A large outbreak of Clostridium difficile-associated disease with an unexpected proportion of deaths and colectomies at a teaching hospital following increased fluoroquinolone use. Infect Control Hosp Epidemiol. 2005;26:273–80. - PubMed
-
- Musher DM, Aslam S, Logan N, et al. Relatively poor outcome after treatment of Clostridium difficile colitis with metronidazole. Clin Infect Dis. 2005;40:1586–90. - PubMed
-
- Pepin J, Alary M-E, Valiquette L, et al. Increasing risk of relapse after treatment of Clostridium difficile colitis in Quebec, Canada. Clin Infect Dis. 2005;40:1591–7. - PubMed
