

Vascular function and the role of oxidative stress in heart failure, heart transplant, and beyond
- PMID: 22753215
- PMCID: PMC3421053
- DOI: 10.1161/HYPERTENSIONAHA.112.193318
Vascular function and the role of oxidative stress in heart failure, heart transplant, and beyond
Abstract
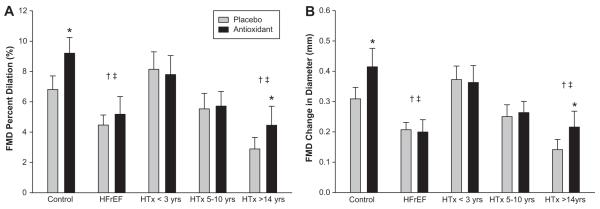
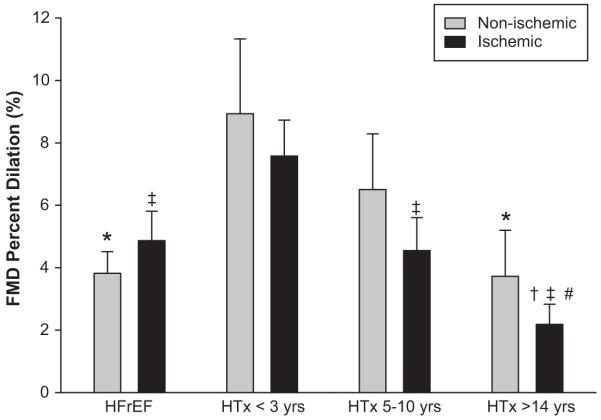
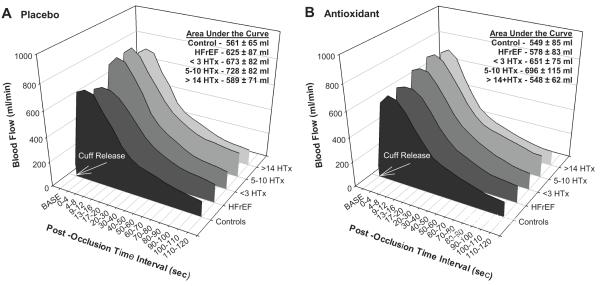
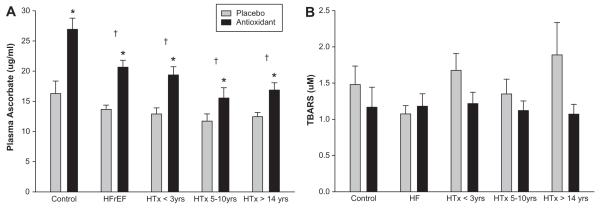
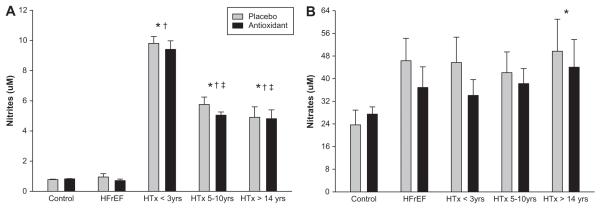
Using flow-mediated vasodilation (FMD), reactive hyperemia, and an acute oral antioxidant cocktail (AOC; vitamins C and E and α-lipoic acid), this study aimed to provide greater insight into altered vascular function and the role of oxidative stress in chronic heart failure patients with reduced ejection fraction (HFrEF) and at several time points beyond heart transplantation (HTx). A total of 61 age-matched subjects (12 healthy controls, 14 New York Heart Association class II and III HFrEF, and 35 HTx recipients [<3 years post-HTx, 5-10 years post-HTx, and >14 years post-HTx]) ingested either placebo (PL) or an AOC before FMD and reactive hyperemia testing of the brachial artery. Vascular function, as measured by FMD, was not different among the controls (6.8±1.9%), recent <3-year post-HTx group (8.1±1.2%), and the 5- to 10-year post-HTx group (5.5±1.0%). However, PL FMD was lower in the HFrEF (4.5±0.7%) and in the >14-year post-HTx group (2.9±0.8%). The AOC increased plasma ascorbate levels in all of the groups but only increased FMD in the controls (PL, 6.8±1.9%; AOC, 9.2±1.0%) and >14-year post-HTx recipients (PL, 2.9±0.8%; AOC, 4.5±1.3%). There were no differences in reactive hyperemia in any of the groups with PL or AOC. This cross-sectional study reveals that, compared with controls, vascular function is blunted in HFrEF, is similar soon after HTx, but is decreased with greater time post-HTx with free radicals implicated in this progression.
Figures

Similar articles
-
Exercise-induced brachial artery vasodilation: effects of antioxidants and exercise training in elderly men.Am J Physiol Heart Circ Physiol. 2010 Feb;298(2):H671-8. doi: 10.1152/ajpheart.00761.2009. Epub 2009 Dec 4. Am J Physiol Heart Circ Physiol. 2010. PMID: 19966056 Free PMC article. Clinical Trial.
-
Chronic antioxidant administration restores macrovascular function in patients with heart failure with reduced ejection fraction.Exp Physiol. 2020 Aug;105(8):1384-1395. doi: 10.1113/EP088686. Epub 2020 Jun 18. Exp Physiol. 2020. PMID: 32495411 Free PMC article.
-
The effect of oral antioxidants on brachial artery flow-mediated dilation following 5 and 10 min of ischemia.Eur J Appl Physiol. 2009 Nov;107(4):445-53. doi: 10.1007/s00421-009-1147-x. Epub 2009 Aug 11. Eur J Appl Physiol. 2009. PMID: 19669786 Clinical Trial.
-
Statin administration improves vascular function in heart failure with preserved ejection fraction.J Appl Physiol (1985). 2024 Apr 1;136(4):877-888. doi: 10.1152/japplphysiol.00775.2023. Epub 2024 Feb 22. J Appl Physiol (1985). 2024. PMID: 38385181 Free PMC article. Clinical Trial.
-
Prevention and rehabilitation after heart transplantation: A clinical consensus statement of the European Association of Preventive Cardiology, Heart Failure Association of the ESC, and the European Cardio Thoracic Transplant Association, a section of ESOT.Eur J Heart Fail. 2024 Sep;26(9):1876-1892. doi: 10.1002/ejhf.3185. Epub 2024 Jun 19. Eur J Heart Fail. 2024. PMID: 38894693
Cited by
-
Exercise training in heart transplantation.World J Transplant. 2021 Nov 18;11(11):466-479. doi: 10.5500/wjt.v11.i11.466. World J Transplant. 2021. PMID: 34868897 Free PMC article. Review.
-
Contrast Ultrasound Assessment of Skeletal Muscle Recruitable Perfusion after Permanent Left Ventricular Assist Device Implantation: Implications for Functional Recovery.J Am Soc Echocardiogr. 2022 May;35(5):495-502. doi: 10.1016/j.echo.2021.12.014. Epub 2021 Dec 29. J Am Soc Echocardiogr. 2022. PMID: 34973393 Free PMC article.
-
Impact of Acute Antioxidant and Tetrahydrobiopterin (BH4) Administration on Locomotor Muscle Microvascular Function in Patients With Heart Failure.Circ Heart Fail. 2025 Jun;18(6):e012446. doi: 10.1161/CIRCHEARTFAILURE.124.012446. Epub 2025 Apr 24. Circ Heart Fail. 2025. PMID: 40270242 Clinical Trial.
-
Vascular function assessed by passive leg movement and flow-mediated dilation: initial evidence of construct validity.Am J Physiol Heart Circ Physiol. 2016 Nov 1;311(5):H1277-H1286. doi: 10.1152/ajpheart.00421.2016. Epub 2016 Sep 16. Am J Physiol Heart Circ Physiol. 2016. PMID: 27638879 Free PMC article.
-
Graft microvascular disease in solid organ transplantation.J Mol Med (Berl). 2014 Aug;92(8):797-810. doi: 10.1007/s00109-014-1173-y. Epub 2014 Jun 1. J Mol Med (Berl). 2014. PMID: 24880953 Free PMC article. Review.
References
-
- Panza JA, Quyyumi AA, Brush JE, Jr., Epstein SE. Abnormal endothelium-dependent vascular relaxation in patients with essential hypertension. N Engl J Med. 1990;323:22–27. - PubMed
-
- Monnink SH, van Haelst PL, van Boven AJ, Stroes ES, Tio RA, Plokker TW, Smit AJ, Veeger NJ, Crijns HJ, van Gilst WH. Endothelial dysfunction in patients with coronary artery disease: A comparison of three frequently reported tests. J Investig Med. 2002;50:19–24. - PubMed
-
- Katz SD, Biasucci L, Sabba C, Strom JA, Jondeau G, Galvao M, Solomon S, Nikolic SD, Forman R, LeJemtel TH. Impaired endothelium-mediated vasodilation in the peripheral vasculature of patients with congestive heart failure. J Am Coll Cardiol. 1992;19:918–925. - PubMed
-
- Drexler H, Hayoz D, Munzel T, Hornig B, Just H, Brunner HR, Zelis R. Endothelial function in chronic congestive heart failure. Am J Cardiol. 1992;69:1596–1601. - PubMed
-
- Celermajer D, Sorensen K, Spiegelhalter D, Georgakopoulos D, Robinson J, Deanfield J. Aging is associated with endothelial dysfunction in healthy men years before the age-related decline in women. J Am Coll Cardiol. 1994;24:471. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
