

Genetically defined subsets of human pancreatic cancer show unique in vitro chemosensitivity
- PMID: 22753594
- PMCID: PMC3513499
- DOI: 10.1158/1078-0432.CCR-12-0827
Genetically defined subsets of human pancreatic cancer show unique in vitro chemosensitivity
Abstract
Purpose: Pancreatic cancer is the fourth cause of death from cancer in the western world. Majority of patients present with advanced unresectable disease responding poorly to most chemotherapeutic agents. Chemotherapy for pancreatic cancer might be improved by adjusting it to individual genetic profiles. We attempt to identify genetic predictors of chemosensitivity to broad classes of anticancer drugs.
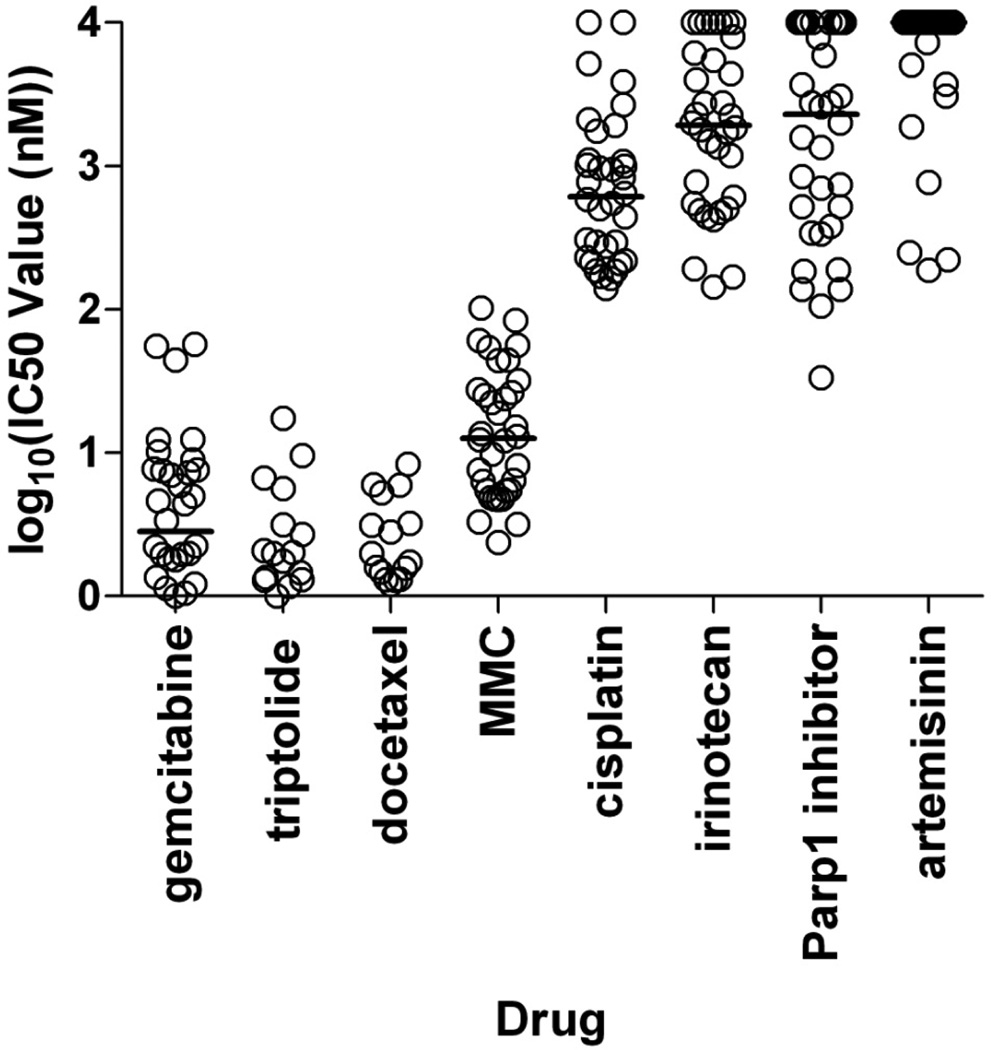
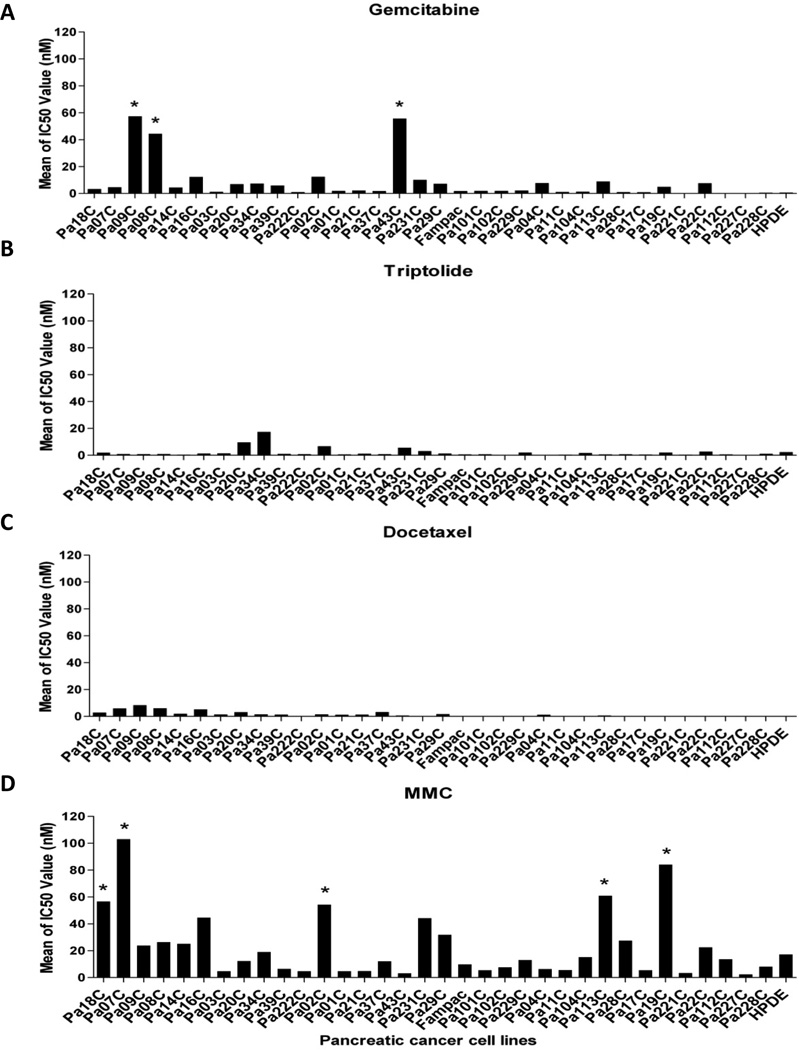
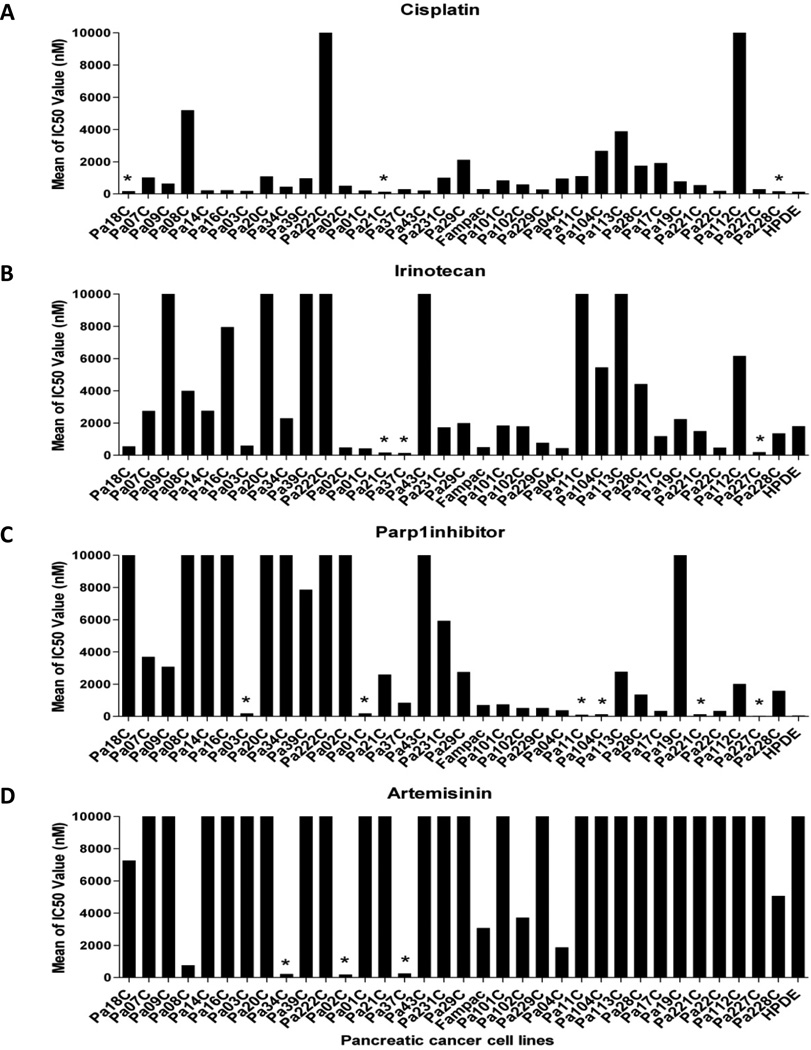
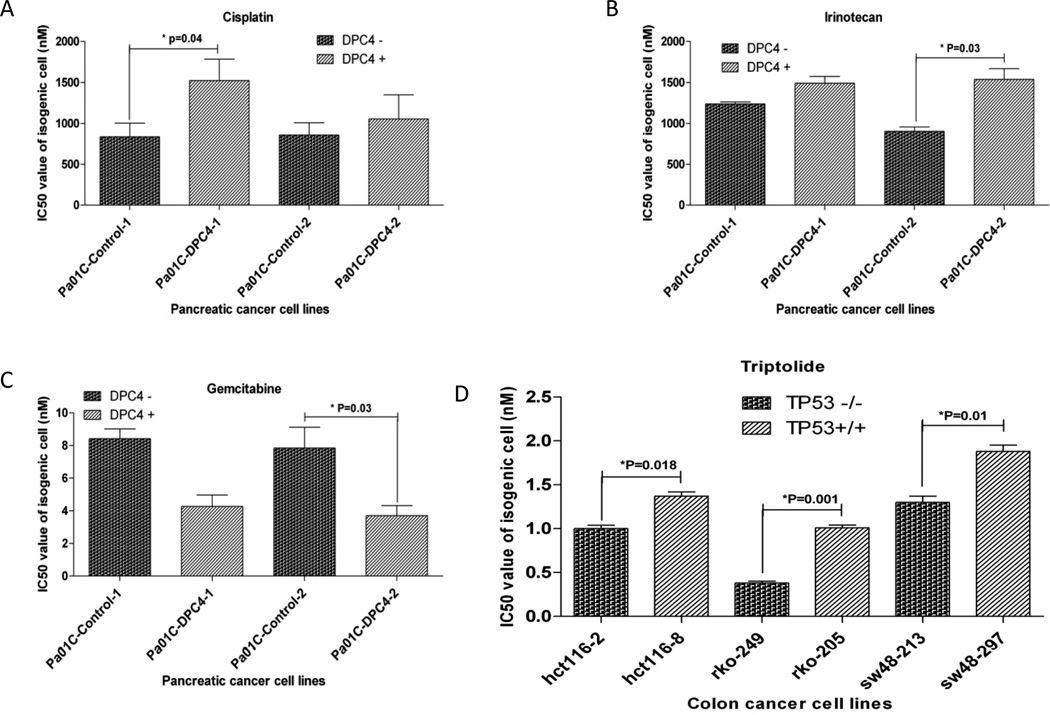
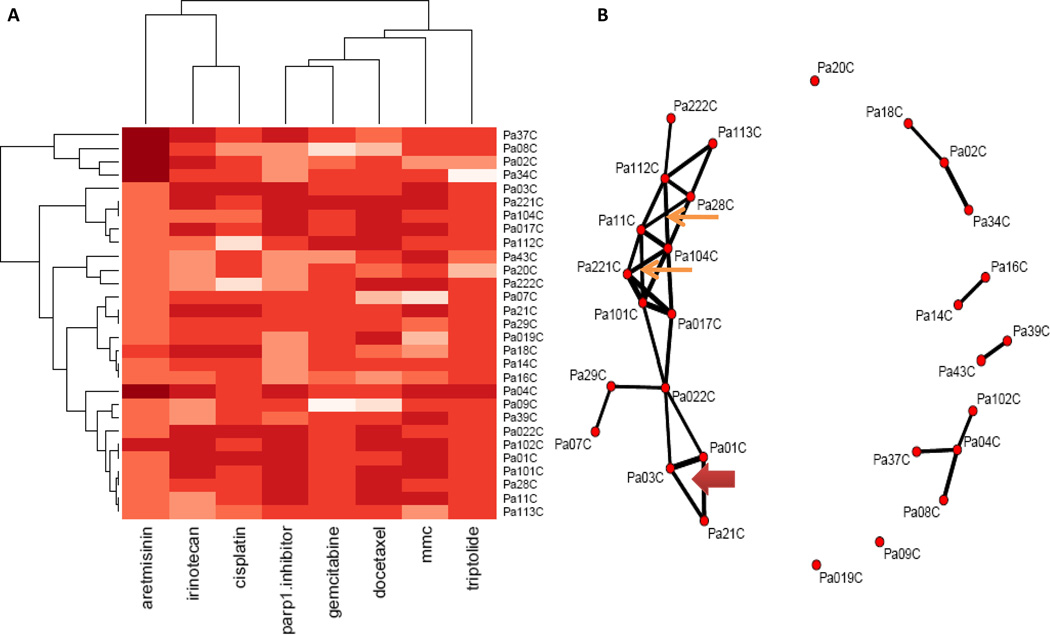
Experimental design: Using a panel of genetically defined human pancreatic cancer cell lines, we tested gemcitabine (antimetabolite), docetaxel (antimicrotubule), mitomycin C (MMC; alkylating), irinotecan (topoisomerase I inhibitor), cisplatin (crosslinking), KU0058948 (Parp1 inhibitor), triptolide (terpenoid drug), and artemisinin (control).
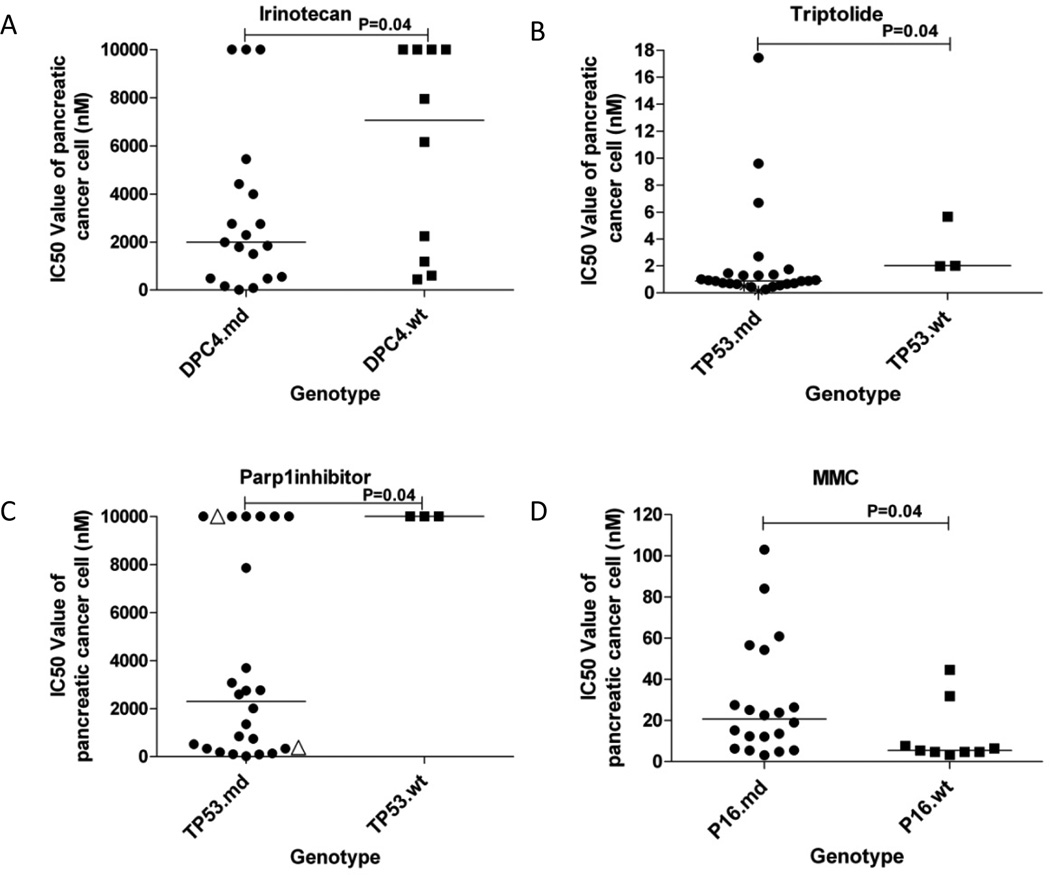
Results: All pancreatic cancer cell lines were sensitive to triptolide and docetaxel. Most pancreatic cancer cells were also sensitive to gemcitabine and MMC. The vast majority of pancreatic cancer cell lines were insensitive to cisplatin, irinotecan, and a Parp1 inhibitor. However, individual cell lines were often sensitive to these compounds in unique ways. We found that DPC4/SMAD4 inactivation sensitized pancreatic cancer cells to cisplatin and irinotecan by 2- to 4-fold, but they were modestly less sensitive to gemcitabine. Pancreatic cancer cells were all sensitive to triptolide and 18% were sensitive to the Parp1 inhibitor. P16/CDKN2A-inactivated pancreatic cancer cells were 3- to 4-fold less sensitive to gemcitabine and MMC.
Conclusions: Chemosensitivity of pancreatic cancer cells correlated with some specific genetic profiles. These results support the hypothesis that genetic subsets of pancreatic cancer exist, and these genetic backgrounds may permit one to personalize the chemotherapy of pancreatic cancer in the future. Further work will need to confirm these responses and determine their magnitude in vivo.
©2012 AACR.
Conflict of interest statement
The authors disclose a patent licensed to Myriad Genetics (Drs. Hruban and Eshleman); Advisory Board membership in Inostics, Morphotek, Exact Sciences and PGDx (Dr. Vogelstein); Ownership Interest in Personal Genome Diagnostics and Inostics (Dr. Diaz); and Advisory Board membership in Roche Molecular Diagnostics (Dr. Eshleman). No potential conflicts of interest were declared by other authors.
Figures
References
-
- Raimondi S, Maisonneuve P, Lowenfels AB. Epidemiology of pancreatic cancer: an overview. Nat Rev Gastroenterol Hepatol. 2009;6:699–708. - PubMed
-
- Shaib YH, Davila JA, El-Serag HB. The epidemiology of pancreatic cancer in the United States: changes below the surface. Aliment Pharmacol Ther. 2006;24:87–94. - PubMed
-
- Burris HA, 3rd, Moore MJ, Andersen J, Green MR, Rothenberg ML, Modiano MR, et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: a randomized trial. J Clin Oncol. 1997;15:2403–2413. - PubMed
-
- Conroy T, Desseigne F, Ychou M, Bouche O, Guimbaud R, Becouarn Y, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 364:1817–1825. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
