

Implementation of cerebral microdialysis at a community-based hospital: A 5-year retrospective analysis
- PMID: 22754722
- PMCID: PMC3385066
- DOI: 10.4103/2152-7806.96868
Implementation of cerebral microdialysis at a community-based hospital: A 5-year retrospective analysis
Abstract
Background: Cerebral microdialysis (MD) provides valuable information about brain metabolism under normal and pathologic conditions. The CMA 600 microdialysis analyzer received US Food and Drug Administration (FDA) approval for clinical use in the United States in 2005. Since then, cerebral MD has been increasingly utilized nationally in the multimodal monitoring of traumatic brain injury (TBI), stroke, aneurysmal subarachnoid hemorrhage, and brain tumors. We describe a 5-year, single-institutional experience using cerebral MD at a community-based hospital, Legacy Emanuel Medical Center (LEMC). Implications for the adoption and utility of MD in medical centers with limited resources are discussed.
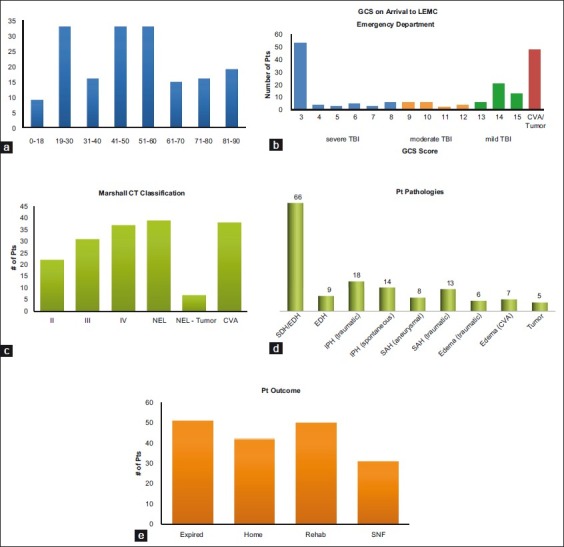
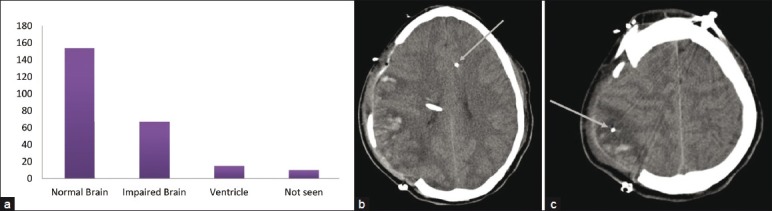
Methods: This is a retrospective chart review and data analysis of 174 consecutive patients who had cerebral MD as part of multimodal brain monitoring. All cerebral MD catheters were placed by board-certified, attending neurosurgeons at LEMC. Clinical severity in the TBI patients was reported using initial Glasgow Coma Scale (GCS); radiologic severity was graded with the Marshall CT grading scale. Measures of the risks of MD placement included post-placement hemorrhage, cerebral infection, and dislodgement.
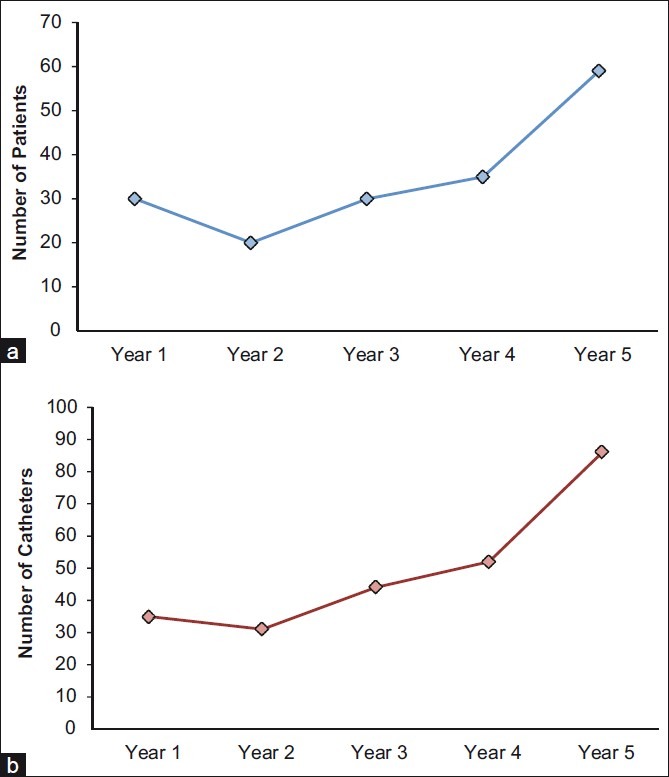
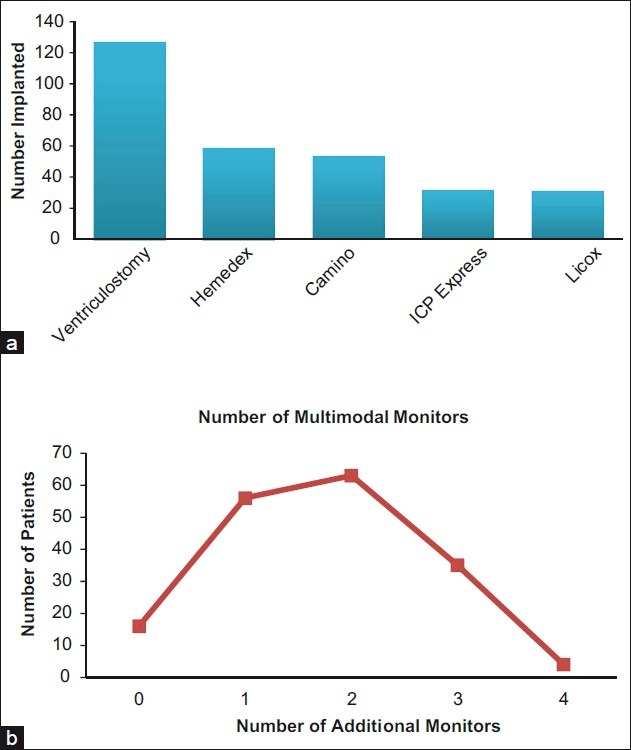
Results: Between July 2005 and July 2010, 248 cerebral MD catheters were placed in 174 patients undergoing multimodal brain monitoring. One hundred and eighty-five catheters were placed at the time of open craniotomy. None were associated with cranial infection. Patients ranged in age from 5 months to 90 years, with a mean of 49 years. The male to female ratio was 1.4:1. The underlying pathologies were: TBI (126), cerebral vascular accident (24), aneurysmal subarachnoid hemorrhage (17), and tumor (7).
Conclusions: Cerebral MD was readily implemented in a community-based hospital. No cerebral hemorrhages or infections were attributed to cerebral MD. Examples of how MD may be a useful adjunct in the clinical decision making of patients with brain injuries are presented.
Keywords: Brain glucose; microdialysis; multimodal brain monitoring; traumatic brain injury.
Figures
Similar articles
-
Technical notes on the placement of cerebral microdialysis: A single center experience.Front Neurol. 2023 Jan 9;13:1041952. doi: 10.3389/fneur.2022.1041952. eCollection 2022. Front Neurol. 2023. PMID: 36698903 Free PMC article.
-
Intracerebral hypoglycemia and its clinical relevance as a prognostic indicator in severe traumatic brain injury: A cerebral microdialysis study from India.Neurol India. 2016 Mar-Apr;64(2):259-64. doi: 10.4103/0028-3886.177617. Neurol India. 2016. PMID: 26954803
-
Translational neurochemical research in acute human brain injury: the current status and potential future for cerebral microdialysis.J Neurotrauma. 2005 Jan;22(1):3-41. doi: 10.1089/neu.2005.22.3. J Neurotrauma. 2005. PMID: 15665601 Review.
-
A Prospective Observational Feasibility Study of Jugular Bulb Microdialysis in Subarachnoid Hemorrhage.Neurocrit Care. 2020 Aug;33(1):241-255. doi: 10.1007/s12028-019-00888-0. Neurocrit Care. 2020. PMID: 31845174
-
[Use of intracerebral microdialysis in severe traumatic brain injury].No Shinkei Geka. 2010 Sep;38(9):795-809. No Shinkei Geka. 2010. PMID: 20864768 Review. Japanese.
Cited by
-
A Review on Microdialysis Calibration Methods: the Theory and Current Related Efforts.Mol Neurobiol. 2017 Jul;54(5):3506-3527. doi: 10.1007/s12035-016-9929-8. Epub 2016 May 17. Mol Neurobiol. 2017. PMID: 27189617 Review.
-
Technical notes on the placement of cerebral microdialysis: A single center experience.Front Neurol. 2023 Jan 9;13:1041952. doi: 10.3389/fneur.2022.1041952. eCollection 2022. Front Neurol. 2023. PMID: 36698903 Free PMC article.
-
Severe Cranioencephalic Trauma: Prehospital Care, Surgical Management and Multimodal Monitoring.Bull Emerg Trauma. 2016 Jan;4(1):8-23. Bull Emerg Trauma. 2016. PMID: 27162922 Free PMC article. Review.
-
Invasive Neuromonitoring Modalities in the Pediatric Population.Neurocrit Care. 2023 Apr;38(2):470-485. doi: 10.1007/s12028-023-01684-7. Epub 2023 Mar 8. Neurocrit Care. 2023. PMID: 36890340 Free PMC article. Review.
-
Update: Microdialysis for Monitoring Cerebral Metabolic Dysfunction after Subarachnoid Hemorrhage.J Clin Med. 2020 Dec 30;10(1):100. doi: 10.3390/jcm10010100. J Clin Med. 2020. PMID: 33396652 Free PMC article. Review.
References
-
- American Hospital Association: Fast Facts on U.S. Hospitals. [cited in 2010]. Available from: http://www.aha.org/research/rc/stat-studies/fast-facts.shtml .
-
- Bellander BM, Cantais E, Enblad P, Hutchinson P, Nordstrom CH, Robertson C, et al. Consensus meeting on microdialysis in neurointensive care. Intensive Care Med. 2004;30:2166–9. - PubMed
-
- Belli A, Sen J, Petzold A, Russo S, Kitchen N, Smith M. Metabolic failure precedes intracranial pressure rises in traumatic brain injury: A microdialysis study. Acta Neuroch (Wien) 2008;150:461–9. discussion 470. - PubMed
-
- Cecil S, Chen PM, Callaway SE, Rowland SM, Adler DE, Chen JW. Traumatic brain injury: Advanced multimodal neuromonitoring from theory to clinical practice. Crit Care Nurse. 2011;31:25–36. quiz 37. - PubMed
-
- Charalambides C, Sgouros S, Sakas D. Intracerebral microdialysis in children. Child's Nerv Syst. 2010;26:215–20. - PubMed
LinkOut - more resources
Full Text Sources
