

Proof of concept for low-dose molecular breast imaging with a dual-head CZT gamma camera. Part II. Evaluation in patients
- PMID: 22755727
- PMCID: PMC3376157
- DOI: 10.1118/1.4719959
Proof of concept for low-dose molecular breast imaging with a dual-head CZT gamma camera. Part II. Evaluation in patients
Abstract
Purpose: Molecular breast imaging (MBI) has shown promise as an adjunct screening technique to mammography for women with dense breasts. The demonstration of reliable lesion detection with MBI performed at low administered doses of Tc-99 m sestamibi, comparable in effective radiation dose to screening mammography, is essential to adoption of MBI for screening. The concept of performing low-dose MBI with dual-head cadmium zinc telluride (CZT) gamma cameras has been investigated in phantoms in Part I. In this work, the objectives were to evaluate the impact of the count sensitivity improvement methods on image quality in patient MBI exams and to determine if adequate lesion detection could be achieved at reduced doses.
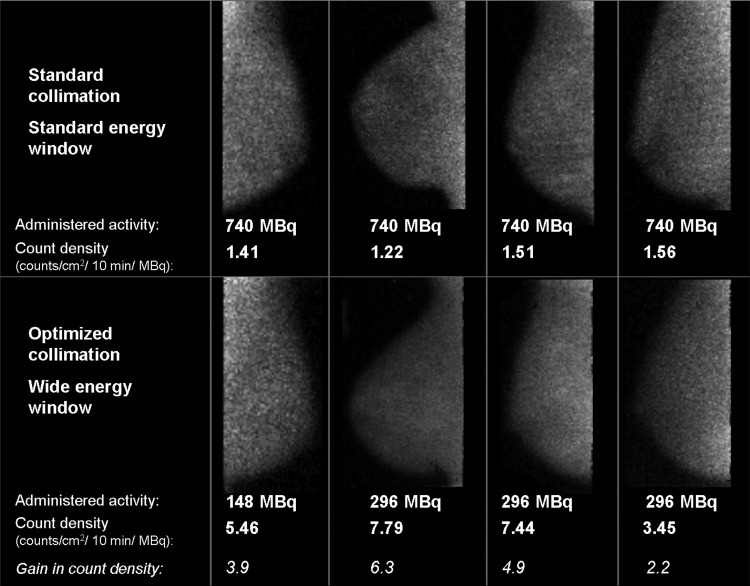
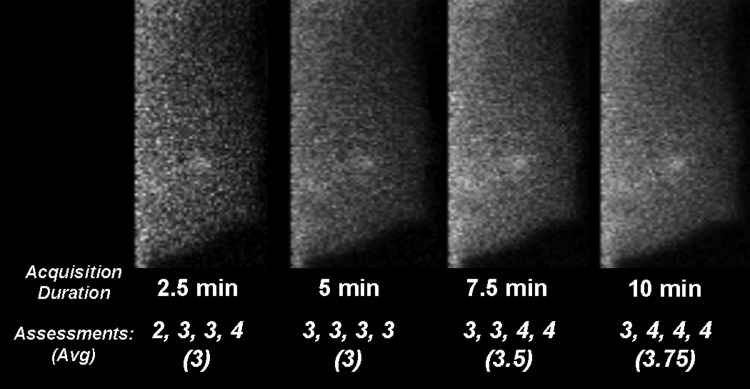
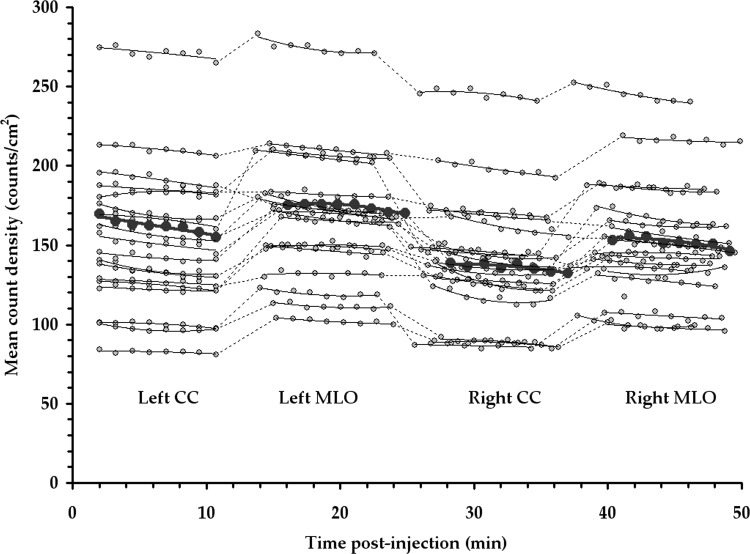
Methods: Following the implementation of two count sensitivity improvement methods, registered collimation optimized for near-field imaging and energy acceptance window optimized for CZT, MBI exams were performed in the course of clinical care. Clinical image count density (counts/cm(2)) was compared between standard MBI [740 MBq (20 mCi) Tc-99 m sestamibi, standard collimation, standard energy window] and low-dose MBI [296 MBq (8 mCi) Tc-99 m sestamibi, optimized collimation, wide energy window] in a cohort of 50 patients who had both types of MBI exams performed. Lesion detection at low doses was evaluated in a separate cohort of 32 patients, in which low-dose MBI was performed following 296 MBq injection and acquired in dynamic mode, allowing the generation of images acquired for 2.5, 5, 7.5, and 10 min/breast view with proportionately reduced count densities. Diagnostic accuracy at each count density level was compared and kappa statistic was used to assess intrareader agreement between 10 min acquisitions and those at shorter acquisition durations.
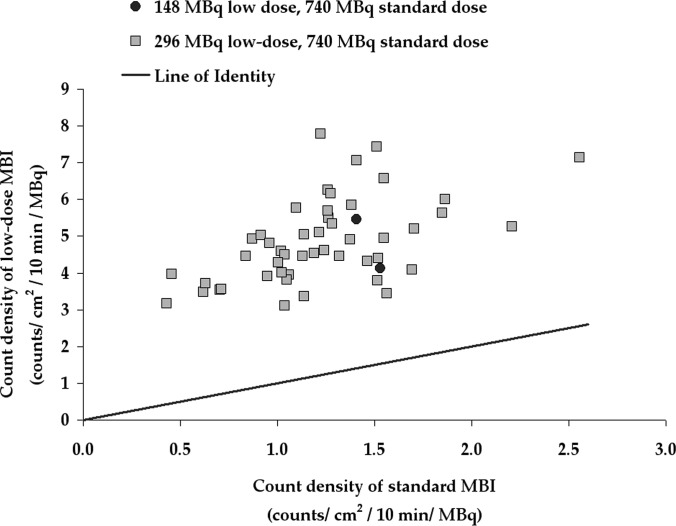
Results: In patient studies, low-dose MBI performed with 296 MBq Tc-99 m sestamibi and new optimal collimation/wide energy window resulted in an average relative gain in count density of 4.2 ± 1.3 compared to standard MBI performed with 740 MBq. Interpretation of low-dose 296 MBq images with count densities corresponding to acquisitions of 2.5, 5, 7.5, and 10 min/view and median lesion size of 1.4 cm resulted in similar diagnostic accuracy across count densities and substantial to near-perfect intrareader agreement between full 10 min-views and lower count density views.
Conclusions: Review of patient studies showed that registered optimized collimation and wide energy window resulted in a substantial gain in count sensitivity as previously indicated by phantom results. This proof of concept work indicates that MBI performed at administered doses of 296 MBq Tc-99 m sestamibi with the applied count sensitivity improvements permits the detection of small breast lesions in patients. Findings suggest that further reductions in acquisition duration or administered dose may be achievable.
© 2012 American Association of Physicists in Medicine.
Figures
References
-
- U.S. Preventive Services Task Force, “Screening for breast cancer: U.S. Preventive Services Task Force recommendation statement,” Ann. Intern. Med. 151, 716–726 (2009). - PubMed
-
- Kolb T. M., Lichy J., and Newhouse J. H., “Comparison of the performance of screening mammography, physical examination, and breast ultrasound and evaluation of factors that influence them: An analysis of 27,825 patient evaluations,” Radiology 225, 165–175 (2002).10.1148/radiol.2251011667 - DOI - PubMed
-
- Carney P. A., Miglioretti D. L., Yankaskas B. C., Kerlikowske K., Rosenberg R., Rutter C. M., Geller B. M., Abraham L. A., Taplin S. H., Dignan M., Cutter G., and Ballard-Barbash R., “Individual and combined effects of age, breast density, and hormone replacement therapy use on the accuracy of screening mammography,” Ann. Intern. Med. 138, 168–175 (2003). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
