

Comparison of the long-term outcomes of kidney transplantation: USA versus Spain
- PMID: 22759384
- PMCID: PMC3616762
- DOI: 10.1093/ndt/gfs287
Comparison of the long-term outcomes of kidney transplantation: USA versus Spain
Abstract
Background: The long-term outcomes of kidney transplantation are suboptimal because many patients lose their allografts or experience premature death. Cross-country comparisons of long-term outcomes of kidney transplantation may provide insight into factors contributing to premature graft failure and death. We evaluated the rates of late graft failure and death among US and Spanish kidney recipients.
Methods: This is a cohort study of US (n = 9609) and Spanish (n = 3808) patients who received a deceased donor kidney transplant in 1990, 1994, 1998 or 2002 and had a functioning allograft 1 year after transplantation with follow-up through September 2006. Ten-year overall and death-censored graft survival and 10-year overall recipient survival and death with graft function (DWGF) were estimated with multivariate Cox models.
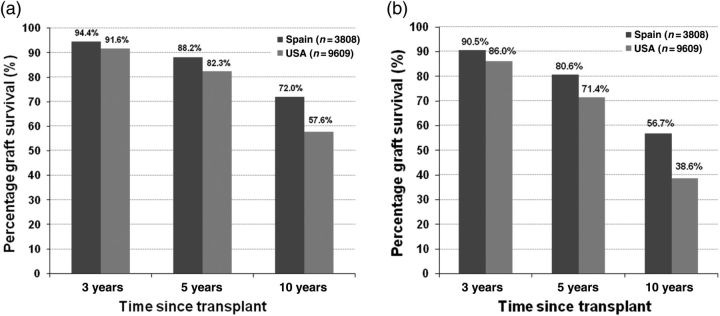
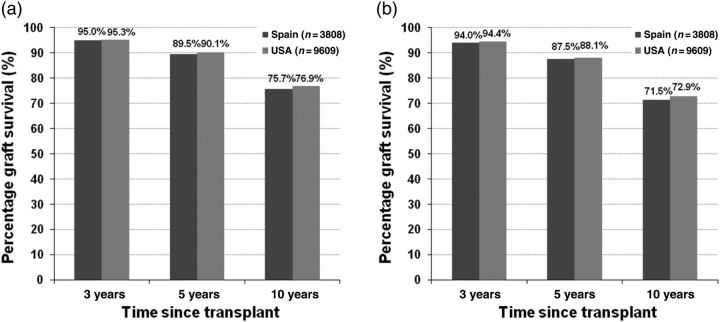
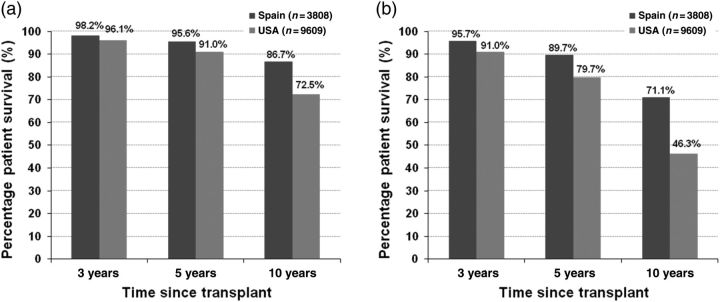
Results: Among recipients alive with graft function 1 year after transplant, the 10-year graft survival was 71.3% for Spanish and 53.4% for US recipients (P < 0.001). The 10-year, death-censored graft survival was 75.6 and 76.0% for Spanish and US recipients, respectively (P = 0.73). The 10-year recipient survival was 86.2% for Spanish and 67.4% for US recipients (P < 0.001). In recipients with diabetes as the cause of ESRD, the adjusted DWGF rates at 10 years were 23.9 and 53.8 per 1000 person-years for Spanish and US recipients, respectively (P < 0.001). Among recipients whose cause of ESRD was not diabetes mellitus, the adjusted 10-year DWGF rates were 11.0 and 25.4 per 1000 person-years for Spanish and US recipients, respectively.
Conclusions: US kidney transplant recipients had more than twice the long-term hazard of DWGF compared with Spanish kidney transplant recipients and similar levels of death-censored graft function. Pre-transplant medical care, comorbidities, such as cardiovascular disease, and their management in each country's health system are possible explanations for the differences between the two countries.
Figures
Comment in
-
Comparing kidney transplant outcomes; caveats and lessons.Nephrol Dial Transplant. 2013 Jan;28(1):9-11. doi: 10.1093/ndt/gfs374. Epub 2012 Sep 17. Nephrol Dial Transplant. 2013. PMID: 22987141 No abstract available.
References
-
- Wolfe RA, Ashby VB, Milford EL, et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant.[see comment] N Engl J Med. 1999;341:1725–1730. doi:10.1056/NEJM199912023412303. - DOI - PubMed
-
- Satayathum S, Pisoni RL, McCullough KP, et al. Kidney transplantation and wait-listing rates from the international Dialysis Outcomes and Practice Patterns Study (DOPPS) Kidney Int. 2005;68:330–337. doi:10.1111/j.1523-1755.2005.00412.x. - DOI - PubMed
-
- Owen WF., Jr Patterns of care for patients with chronic kidney disease in the United States: dying for improvement. J Am Soc Nephrol. 2003;14:S76–S80. doi:10.1097/01.ASN.0000070145.00225.EC. - DOI - PubMed
-
- Alexander GC, Sehgal AR. Barriers to cadaveric renal transplantation among blacks, women and the poor. J Am Med Assoc. 1998;280:1148–1152. doi:10.1001/jama.280.13.1148. - DOI - PubMed
-
- Goodkin DA, Bragg-Gresham JL, Koenig KG, et al. Association of comorbid conditions and mortality in hemodialysis patients in Europe, Japan, and the United States: the Dialysis Outcomes and Practice Patterns Study (DOPPS) J Am Soc Nephrol. 2003;14:3270–3277. doi:10.1097/01.ASN.0000100127.54107.57. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
