

The diameter of the originating vein determines esophageal and gastric fundic varices in portal hypertension secondary to posthepatitic cirrhosis
- PMID: 22760900
- PMCID: PMC3370313
- DOI: 10.6061/clinics/2012(06)11
The diameter of the originating vein determines esophageal and gastric fundic varices in portal hypertension secondary to posthepatitic cirrhosis
Abstract
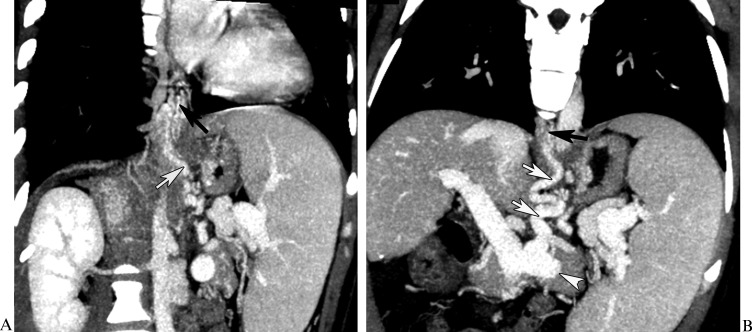
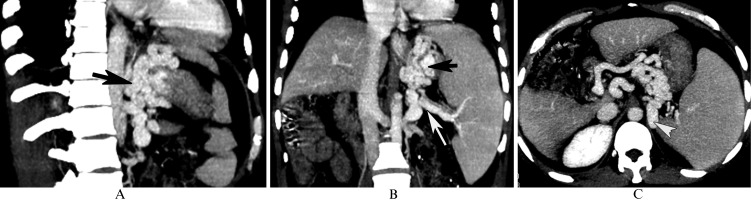
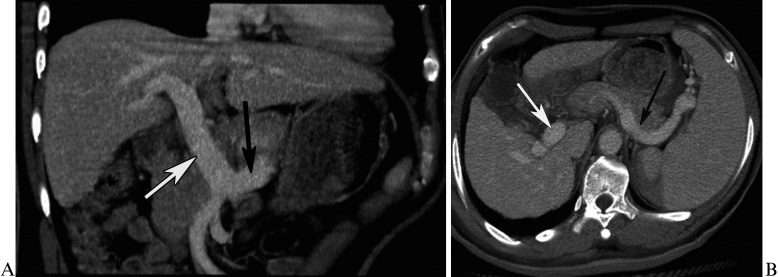
Objective: The aim of this study was to determine whether and how the diameter of the vein that gives rise to the inflowing vein of the esophageal and gastric fundic varices secondary to posthepatitic cirrhosis, as measured with multidetector-row computed tomography, could predict the varices and their patterns.
Methods: A total of 106 patients with posthepatitic cirrhosis underwent multidetector-row computed tomography. Patients with and without esophageal and gastric fundic varices were enrolled in Group 1 and Group 2, respectively. Group 1 was composed of Subgroup A, consisting of patients with varices, and Subgroup B consisted of patients with varices in combination with portal vein-inferior vena cava shunts. The diameters of the originating veins of veins entering the varices were reviewed and statistically analyzed.
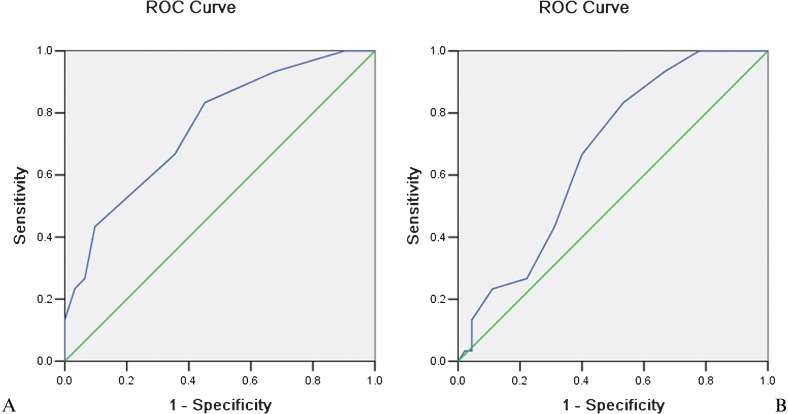
Results: The originating veins were the portal vein in 8% (6/75) of patients, the splenic vein in 65.3% (49/75) of patients, and both the portal and splenic veins in 26.7% (20/75) of patients. The splenic vein diameter in Group 1 was larger than that in Group 2, whereas no differences in portal vein diameters were found between groups. In Group 1, the splenic vein diameter in Subgroup A was larger than that in Subgroup B. A cut-off splenic vein diameter of 8.5 mm achieved a sensitivity of 83.3% and specificity of 58.1% for predicting the varices. For discrimination of the varices in combination with and without portal vein-inferior vena cava shunts, a cut-off diameter of 9.5 mm achieved a sensitivity of 66.7% and specificity of 60.0%.
Conclusion: The diameter of the splenic vein can be used to predict esophageal and gastric fundic varices and their patterns.
Conflict of interest statement
No potential conflict of interest was reported.
Figures
Similar articles
-
Evaluation of entire gastric fundic and esophageal varices secondary to posthepatitic cirrhosis: portal venography using 64-row MDCT.Abdom Imaging. 2010 Feb;35(1):1-7. doi: 10.1007/s00261-009-9506-y. Epub 2009 Feb 27. Abdom Imaging. 2010. PMID: 19247703
-
Correlation of splenic volume with hematological parameters, splenic vein diameter, portal pressure and grade of varices in extrahepatic portal vein obstruction in children.Pediatr Surg Int. 2011 May;27(5):467-71. doi: 10.1007/s00383-010-2847-3. Pediatr Surg Int. 2011. PMID: 21243364
-
[Portal venography with 64-slice MDCT in evaluation of the anatomic distribution of compensatory circulation resulting from posthepatitic cirrhosis].Sheng Wu Yi Xue Gong Cheng Xue Za Zhi. 2010 Jun;27(3):511-5. Sheng Wu Yi Xue Gong Cheng Xue Za Zhi. 2010. PMID: 20649008 Chinese.
-
Is portal vein cavernous transformation a component of congenital hepatic fibrosis?World J Gastroenterol. 2007 Apr 7;13(13):1928-9. doi: 10.3748/wjg.v13.i13.1928. World J Gastroenterol. 2007. PMID: 17461491 Free PMC article. Review.
-
Etiologies of Splenic Venous Hypertension: A Review.J Clin Transl Hepatol. 2024 Jun 28;12(6):594-606. doi: 10.14218/JCTH.2024.00054. Epub 2024 May 20. J Clin Transl Hepatol. 2024. PMID: 38974953 Free PMC article. Review.
Cited by
-
CT-based nomogram predicts esophageal gastric variceal bleeding in noncirrhotic portal hypertension caused by hepatic schistosomiasis.BMC Med Inform Decis Mak. 2025 Jan 7;25(1):8. doi: 10.1186/s12911-024-02777-9. BMC Med Inform Decis Mak. 2025. PMID: 39773170 Free PMC article.
-
Quantitative measurements of esophageal varices using computed tomography for prediction of severe varices and the risk of bleeding: a preliminary study.Insights Imaging. 2022 Mar 14;13(1):47. doi: 10.1186/s13244-022-01189-5. Insights Imaging. 2022. PMID: 35286491 Free PMC article.
-
A novel scoring system for prediction of esophageal varices in critically ill patients.Clin Exp Gastroenterol. 2017 Dec 7;10:315-325. doi: 10.2147/CEG.S144700. eCollection 2017. Clin Exp Gastroenterol. 2017. PMID: 29263686 Free PMC article.
-
Clinical Analysis of Sinistral Portal Hypertension.Iran J Med Sci. 2024 Aug 1;49(8):487-493. doi: 10.30476/ijms.2023.99570.3164. eCollection 2024 Aug. Iran J Med Sci. 2024. PMID: 39205819 Free PMC article.
-
Multiparametric radiomics nomogram may be used for predicting the severity of esophageal varices in cirrhotic patients.Ann Transl Med. 2020 Mar;8(5):186. doi: 10.21037/atm.2020.01.122. Ann Transl Med. 2020. PMID: 32309333 Free PMC article.
References
-
- Pinzani M, Rosselli M, Zuckermann M. Liver cirrhosis. Best Pract Res Clin Gastroenterol. 2011;25(2):281–90. - PubMed
-
- Iwakiri Y, Groszmann RJ. The hyperdynamic circulation of chronic liver diseases: from the patient to the molecule. Hepatology. 2006;43(2 Suppl 1) :S121–31. - PubMed
-
- Garini G, Delsante M, Iannuzzella F. Pathophysiology of portal hypertension and mechanisms of sodium and water retention in cirrhosis. Recenti Prog Med. 2011;102(3):134–40. - PubMed
-
- Nazyrov FG, Deviatov AV, Babadzhanov AKh, Sultanov SA. Specific development and course of portal hypertension complication in patients with hepatic cirrhosis of HBV and HCV etiology. Vestn Khir Im I I Grek. 2011;170(1):22–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
