

An ecological study on the geographic patterns of ischaemic heart disease in Portugal and its association with demography, economic factors and health resources distribution
- PMID: 22761279
- PMCID: PMC3391373
- DOI: 10.1136/bmjopen-2011-000595
An ecological study on the geographic patterns of ischaemic heart disease in Portugal and its association with demography, economic factors and health resources distribution
Abstract
Objectives: Being one of the main causes of morbidity and mortality in developed countries, ischaemic heart disease's (IHD) incidence and mortality present clear differences between and within countries. Several authors already proposed possible explanations based on the demography, environmental factors, diet and level of urbanisation. This study reflects the Portuguese reality concerning IHD, by analysing the geographical distribution of hospital admissions and mortality due to this condition, in Portugal, and its association with demography, economical factors and the distribution of healthcare resources at the regional level.
Design: Ecological study.
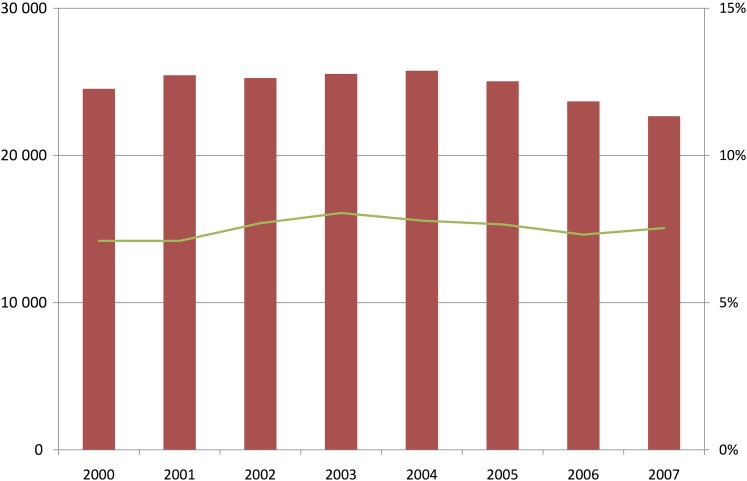
Setting: Data from all Portuguese Public Hospitals were obtained using the National Registry of Hospital Admissions, between 2000 and 2007, and data on demography, economical factors and health resources distribution were obtained from the National Institute of Statistics.
Participants: Aggregated statistics on hospital admissions and mortality were computed for 278 counties based on almost 200 000 admissions.
Primary and secondary outcome measures: Mortality rate; hospital admissions rate.
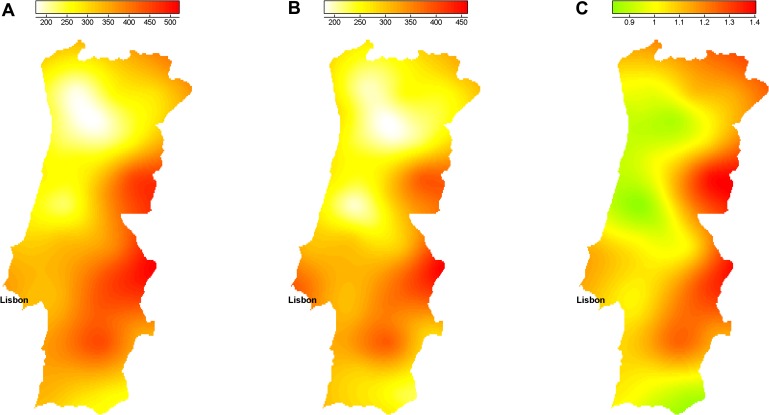
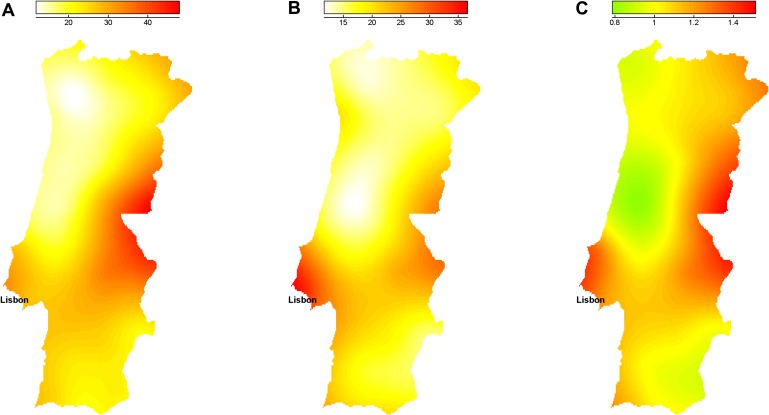
Results: The geographical distribution of non-adjusted mortality and hospital admission showed an inner/coastal pattern but no North/South gradient was clear. Counties with higher economical development had significantly higher mortality and admission rates. However, healthcare resources distribution was not significantly associated with IHD hospital admission and mortality. When adjusted for age, gender, economic development and health resources distribution, there was still unexplained geographical variation both in hospital admissions and mortality rates.
Conclusion: A pattern in the geographic distribution of incidence and mortality of IHD was clear even after the adjustment for age and gender. Economical variables were the ones presenting the strongest association. These types of analysis may be very helpful for the definition of health policies, in particular to identify priority regions for disease prevention and guidelines for healthcare resources distribution.
Conflict of interest statement
Figures
Similar articles
-
[State of health of populations residing in geothermal areas of Tuscany].Epidemiol Prev. 2012 Sep-Oct;36(5 Suppl 1):1-104. Epidemiol Prev. 2012. PMID: 23139155 Italian.
-
Effects of short-term exposure to air pollution on hospital admissions of young children for acute lower respiratory infections in Ho Chi Minh City, Vietnam.Res Rep Health Eff Inst. 2012 Jun;(169):5-72; discussion 73-83. Res Rep Health Eff Inst. 2012. PMID: 22849236
-
Ischaemic Heart Disease at the University Hospital of the West Indies: Trends in Hospital Admissions and Inpatient Mortality Rates 2005-2010.West Indian Med J. 2014 Sep;63(5):424-30. doi: 10.7727/wimj.2013.293. Epub 2014 May 8. West Indian Med J. 2014. PMID: 25781277 Free PMC article.
-
[SENTIERI - Epidemiological Study of Residents in National Priority Contaminated Sites. Sixth Report].Epidemiol Prev. 2023 Jan-Apr;47(1-2 Suppl 1):1-286. doi: 10.19191/EP23.1-2-S1.003. Epidemiol Prev. 2023. PMID: 36825373 Italian.
-
The effect of exposure to long working hours on ischaemic heart disease: A systematic review and meta-analysis from the WHO/ILO Joint Estimates of the Work-related Burden of Disease and Injury.Environ Int. 2020 Sep;142:105739. doi: 10.1016/j.envint.2020.105739. Epub 2020 Jun 5. Environ Int. 2020. PMID: 32505014 Free PMC article.
Cited by
-
Geographic Variation in Top-10 Prescribed Medicines and Potentially Inappropriate Medication in Portugal: An Ecological Study of 2.2 Million Older Adults.Int J Environ Res Public Health. 2022 Oct 10;19(19):12938. doi: 10.3390/ijerph191912938. Int J Environ Res Public Health. 2022. PMID: 36232238 Free PMC article.
-
Patient and hospital determinants of primary percutaneous coronary intervention in England, 2003-2013.Heart. 2016 Feb 15;102(4):313-319. doi: 10.1136/heartjnl-2015-308616. Epub 2016 Jan 5. Heart. 2016. PMID: 26732182 Free PMC article.
-
Healthcare Equity and Commissioning: A Four-Year National Analysis of Portuguese Primary Healthcare Units.Int J Environ Res Public Health. 2022 Nov 10;19(22):14819. doi: 10.3390/ijerph192214819. Int J Environ Res Public Health. 2022. PMID: 36429538 Free PMC article.
References
-
- Muller-Nordhorn J, Binting S, Roll S, et al. An update on regional variation in cardiovascular mortality within Europe. Eur Heart J 2008;29:1316–26 - PubMed
-
- Sans S, Kesteloot H, Kromhout D. The burden of cardiovascular diseases mortality in Europe. Task Force of the European Society of Cardiology on cardiovascular mortality and morbidity statistics in Europe. Eur Heart J 1997;18:1231–48 - PubMed
-
- Andersohn F, Schlattmann P, Roll S, et al. Regional variation of mortality from ischemic heart disease in Germany from 1998 to 2007. Clin Res Cardiol 2010;99:511–18 - PubMed
-
- Marrugat J, Elosua R, Aldasoro E, et al. Regional variability in population acute myocardial infarction cumulative incidence and mortality rates in Spain 1997 and 1998. Eur J Epidemiol 2004;19:831–9 - PubMed
-
- Morris RW, Whincup PH, Emberson JR, et al. North-south gradients in Britain for stroke and CHD: are they explained by the same factors? Stroke 2003;34:2604–9 - PubMed
LinkOut - more resources
Full Text Sources
Molecular Biology Databases