

High prevalence of tuberculosis and serious bloodstream infections in ambulatory individuals presenting for antiretroviral therapy in Malawi
- PMID: 22761767
- PMCID: PMC3382251
- DOI: 10.1371/journal.pone.0039347
High prevalence of tuberculosis and serious bloodstream infections in ambulatory individuals presenting for antiretroviral therapy in Malawi
Abstract
Background: Tuberculosis (TB) and serious bloodstream infections (BSI) may contribute to the high early mortality observed among patients qualifying for antiretroviral therapy (ART) with unexplained weight loss, chronic fever or chronic diarrhea.
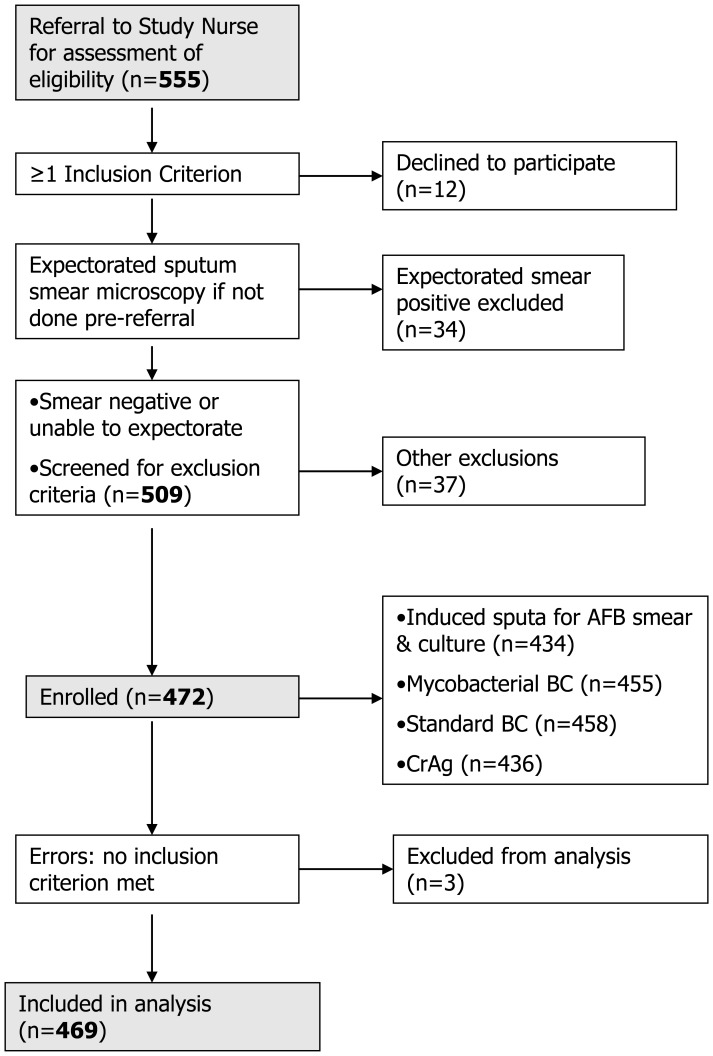
Methods and findings: A prospective cohort study determined the prevalence of undiagnosed TB or BSI among ambulatory HIV-infected adults with unexplained weight loss and/or chronic fever, or diarrhea in two routine program settings in Malawi. Subjects with positive expectorated sputum smears for AFB were excluded. Investigations Bacterial and mycobacterial blood cultures, cryptococcal antigen test (CrAg), induced sputum (IS) for TB microscopy and solid culture, full blood count and CD4 lymphocyte count. Among 469 subjects, 52 (11%) had microbiological evidence of TB; 50 (11%) had a positive (non-TB) blood culture and/or positive CrAg. Sixty-five additional TB cases were diagnosed on clinical and radiological grounds. Nontyphoidal Salmonellae (NTS) were the most common blood culture pathogens (29 cases; 6% of participants and 52% of bloodstream isolates). Multivariate analysis of baseline clinical and hematological characteristics found significant independent associations between oral candidiasis or lymphadenopathy and TB, marked CD4 lymphopenia and NTS infection, and severe anemia and either infection, but low positive likelihood ratios (<2 for all combinations).
Conclusions: We observed a high prevalence of TB and serious BSI, particularly NTS, in a program cohort of chronically ill HIV-infected outpatients. Baseline clinical and hematological characteristics were inadequate predictors of infection. HIV clinics need better rapid screening tools for TB and BSI. Clinical trials to evaluate empiric TB or NTS treatment are required in similar populations.
Conflict of interest statement
References
-
- Braitstein P, Brinkhof MW, Dabis F, Schechter M, Boulle A, et al. Mortality of HIV-1-infected patients in the first year of antiretroviral therapy: comparison between low-income and high-income countries. Lancet. 2006;367:817–824. - PubMed
-
- Lawn SD, Myer L, Orrell C, Bekker LG, Wood R. Early mortality among adults accessing a community-based antiretroviral service in South Africa: implications for programme design. AIDS. 2005;19:2141–2148. - PubMed
-
- Ngoma D, Makombe SD, Kamoto K, Harries AD. World Health Organization Clinical Stage 3 disease conditions in HIV-infected patients who start antiretroviral therapy in Malawi. Trop Doct. 2008;38:159–160. - PubMed
-
- Stringer JS, Zulu I, Levy J, Stringer EM, Mwango A, et al. Rapid scale-up of antiretroviral therapy at primary care sites in Zambia: feasibility and early outcomes. JAMA. 2006;296:782–793. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
