

Attrition among human immunodeficiency virus (HIV)- infected patients initiating antiretroviral therapy in China, 2003-2010
- PMID: 22761787
- PMCID: PMC3384674
- DOI: 10.1371/journal.pone.0039414
Attrition among human immunodeficiency virus (HIV)- infected patients initiating antiretroviral therapy in China, 2003-2010
Abstract
Background: Mortality and morbidity from HIV have dramatically decreased in both high- and low-income countries. However, some patients may not benefit from combination antiretroviral therapy (cART) because of inadequate access to HIV care, including attrition after care initiation.
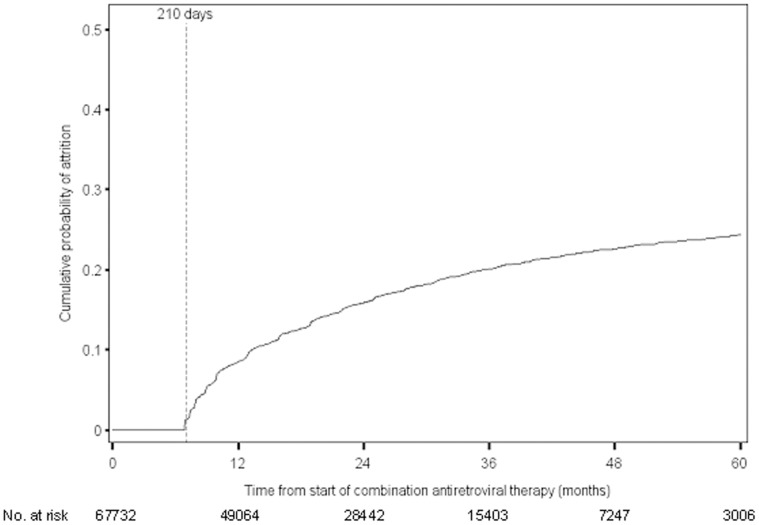
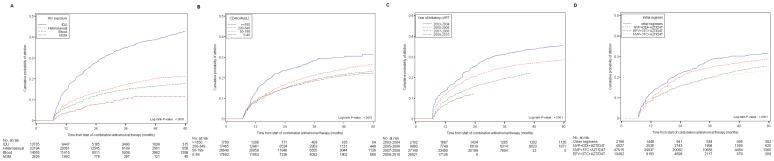
Methodology/principal findings: The study population included all HIV-infected patients receiving cART through the Chinese National Free Antiretroviral Treatment Program from 1 January 2003 to 31 December 2010 (n = 106,542). We evaluated retention in HIV care and used multivariable Cox proportional hazard models to identify independent factors predictive of attrition. The cumulative probability of attrition from cART initiation was 9% at 12 months, 13% at 18 months, 16% at 24 months and 24% at 60 months. A number of factors were associated with attrition, including younger age, male gender, and being single or divorced. Patients with higher CD4 cell counts at cART initiation were more likely to drop out of HIV care. The proportion of patients remaining in HIV care increased in more recent calendar years and among patients who initiated modern cART regimens.
Conclusions/significance: Retention in HIV care is essential for optimizing individual and public health outcomes. Attrition, even the degree observed in our study, can lead to premature morbidity and mortality, and possibly affect further transmission of HIV and HIV resistant drug variants. Effective strategies to promote retention in HIV care programs are needed. In China these strategies may include focusing particularly on younger male patients and those with higher CD4 cell counts at therapy initiation.
Conflict of interest statement
Figures
Similar articles
-
Decreasing excess mortality of HIV-infected patients initiating antiretroviral therapy: comparison with mortality in general population in China, 2003-2009.J Acquir Immune Defic Syndr. 2013 Aug 15;63(5):e150-7. doi: 10.1097/QAI.0b013e3182948d82. J Acquir Immune Defic Syndr. 2013. PMID: 23572014 Free PMC article.
-
Outcomes of second-line combination antiretroviral therapy for HIV-infected patients: a cohort study from Rio de Janeiro, Brazil.BMC Infect Dis. 2014 Dec 19;14:699. doi: 10.1186/s12879-014-0699-5. BMC Infect Dis. 2014. PMID: 25523385 Free PMC article.
-
Risk of discontinuation of nevirapine due to toxicities in antiretroviral-naive and -experienced HIV-infected patients with high and low CD4+ T-cell counts.Antivir Ther. 2007;12(3):325-33. Antivir Ther. 2007. PMID: 17591022 Clinical Trial.
-
[National consensus document by GESIDA/National Aids Plan on antiretroviral treatment in adults infected by the human immunodeficiency virus (January 2011 update)].Enferm Infecc Microbiol Clin. 2011 Mar;29(3):209.e1-103. doi: 10.1016/j.eimc.2010.12.004. Enferm Infecc Microbiol Clin. 2011. PMID: 21388714 Spanish.
-
[Progress on influencing factors of late diagnosis in HIV-infected patients].Zhonghua Liu Xing Bing Xue Za Zhi. 2024 Feb 10;45(2):313-318. doi: 10.3760/cma.j.cn112338-20230908-00142. Zhonghua Liu Xing Bing Xue Za Zhi. 2024. PMID: 38413074 Review. Chinese.
Cited by
-
Retention and risk factors for attrition in a large public health ART program in Myanmar: a retrospective cohort analysis.PLoS One. 2014 Sep 30;9(9):e108615. doi: 10.1371/journal.pone.0108615. eCollection 2014. PLoS One. 2014. PMID: 25268903 Free PMC article.
-
HIV-1 Treatment-as-Prevention: A Cohort Study Analysis of Serodiscordant Couples in Rural Southwest China.Medicine (Baltimore). 2015 Jun;94(24):e902. doi: 10.1097/MD.0000000000000902. Medicine (Baltimore). 2015. PMID: 26091454 Free PMC article. Clinical Trial.
-
Mortality and Attrition Rates within the First Year of Antiretroviral Therapy Initiation among People Living with HIV in Guangxi, China: An Observational Cohort Study.Biomed Res Int. 2021 Feb 10;2021:6657112. doi: 10.1155/2021/6657112. eCollection 2021. Biomed Res Int. 2021. PMID: 33628803 Free PMC article. Clinical Trial.
-
Retention of Adult Patients on Antiretroviral Therapy in Low- and Middle-Income Countries: Systematic Review and Meta-analysis 2008-2013.J Acquir Immune Defic Syndr. 2015 May 1;69(1):98-108. doi: 10.1097/QAI.0000000000000553. J Acquir Immune Defic Syndr. 2015. PMID: 25942461 Free PMC article.
-
HIV Drug Resistance Mutations Detection by Next-Generation Sequencing during Antiretroviral Therapy Interruption in China.Pathogens. 2021 Feb 25;10(3):264. doi: 10.3390/pathogens10030264. Pathogens. 2021. PMID: 33668946 Free PMC article.
References
-
- Gilks CF, Crowley S, Ekpini R, Gove S, Perriens J, et al. The WHO public-health approach to antiretroviral treatment against HIV in resource-limited settings. Lancet. 2006;368:505–510. - PubMed
-
- Zhang F, Dou Z, Ma Y, Zhang Y, Zhao Y, et al. Effect of earlier initiation of antiretroviral treatment and increased treatment coverage on HIV-related mortality in China: a national observational cohort study. Lancet Infect Dis. 2010;11:516–524. - PubMed
-
- Zhang F, Dou Z, Ma Y, Zhao Y, Liu Z, et al. Five-year outcomes of the China National Free Antiretroviral Treatment Program. Ann Intern Med 151: 241–251, W-252. 2009. - PubMed
-
- Braitstein P, Brinkhof MW, Dabis F, Schechter M, Boulle A, et al. Mortality of HIV-1-infected patients in the first year of antiretroviral therapy: comparison between low-income and high-income countries. Lancet. 2006;367:817–824. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
