

Preoperative transarterial Embolisation in bone tumors
- PMID: 22761978
- PMCID: PMC3386530
- DOI: 10.4329/wjr.v4.i5.186
Preoperative transarterial Embolisation in bone tumors
Abstract
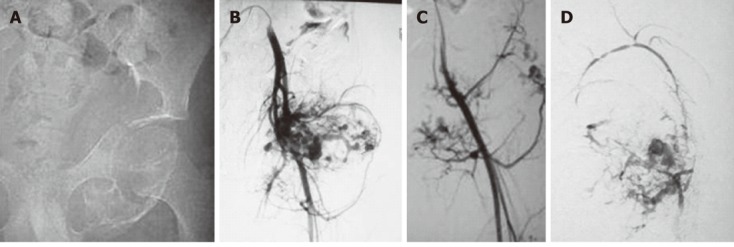
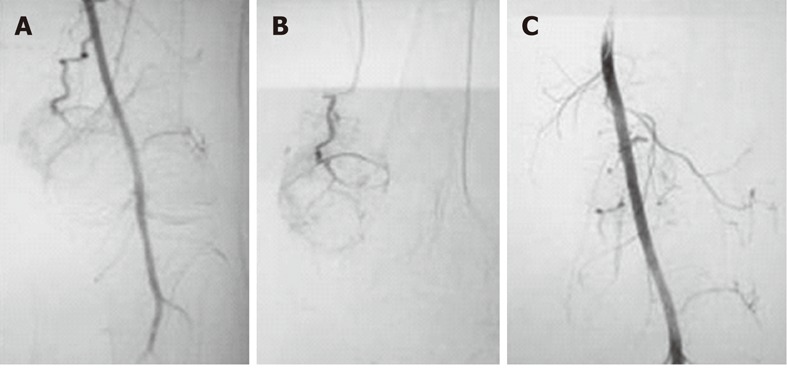
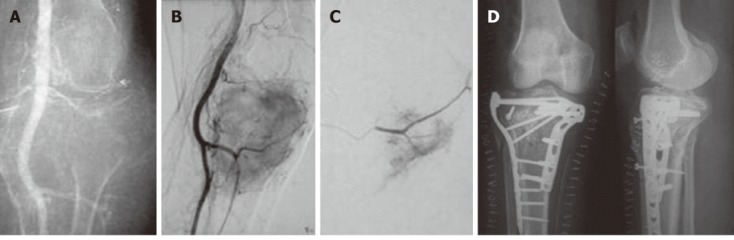
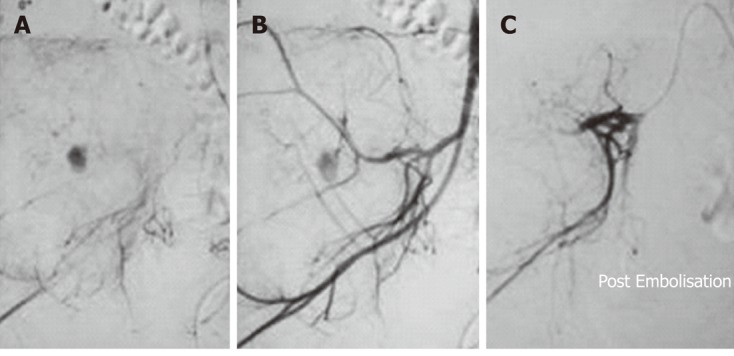
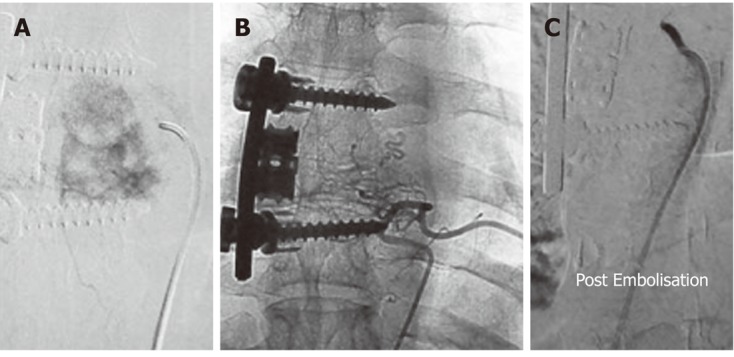
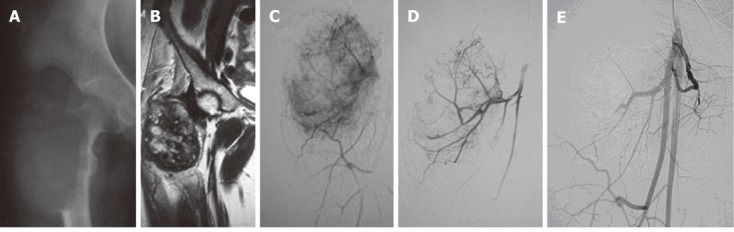
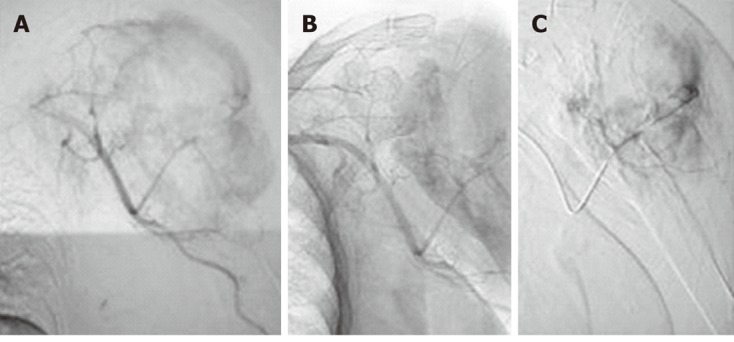
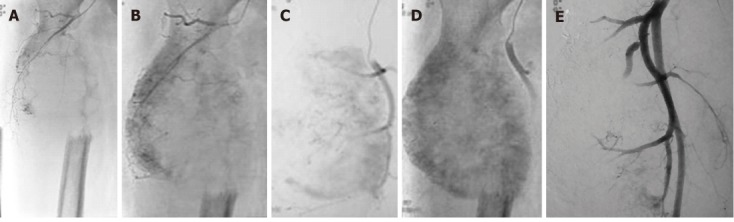
Bone tumors include a variety of lesions, both primary and metastatic. The treatment modalities for bone tumors vary with the individual lesion, but in general surgical excision is the treatment of choice with other adjunctive therapies. However, surgery for many bone tumors is complex due to several factors including tumor bulk, vascularity, vicinity to vital structures and potentially inaccessible location of the lesion. Transarterial Embolisation (TAE) is one of the important adjuvant treatment modalities and in some cases it may be the primary and curative treatment. Preoperative TAE has proved to be effective in both primary and metastatic bone tumors. It reduces tumor vascularity and intraoperative blood loss, the need for blood transfusion and associated complications, allows better definition of tissue planes at surgery affording more complete excision, and hence reduced recurrence. Preoperative chemoEmbolisation has also been shown to increase the sensitivity of some tumors to subsequent chemotherapy and radiotherapy. There are several techniques and embolic agents available for this purpose, but the ultimate aim is to achieve tumor devascularization. In this review, we discuss the techniques including the choice of embolic agent, application to individual lesions and potential complications.
Keywords: Blood loss; Bone tumors; Embolisation; Interventional; Radiology; Surgical.
Figures
References
-
- Börüban S, Sancak T, Yildiz Y, Sağlik Y. Embolisation of benign and malignant bone and soft tissue tumors of the extremities. Diagn Interv Radiol. 2007;13:164–171. - PubMed
-
- Kauffmann G, Wimmer B, Bischoff W, Adler C, Strecker EP. [Fundamental experiments for therapeutic artery occlusion by angiography catheters (author’s transl)] Radiologe. 1977;17:489–491. - PubMed
-
- Radeleff B, Eiers M, Lopez-Benitez R, Noeldge G, Hallscheidt P, Grenacher L, Libicher M, Zeifang F, Meeder PJ, Kauffmann GW, et al. Transarterial Embolisation of primary and secondary tumors of the skeletal system. Eur J Radiol. 2006;58:68–75. - PubMed
-
- Brado M, Hansmann HJ, Richter GM, Kauffmann GW. [Interventional therapy of primary and secondary tumors of the spine] Orthopade. 1998;27:269–273. - PubMed
-
- Munk PL, Legiehn GM. Musculoskeletal interventional radiology: applications to oncology. Semin Roentgenol. 2007;42:164–174. - PubMed
LinkOut - more resources
Full Text Sources
