

Comparison of DWI and PET/CT in evaluation of lymph node metastasis in uterine cancer
- PMID: 22761980
- PMCID: PMC3386532
- DOI: 10.4329/wjr.v4.i5.207
Comparison of DWI and PET/CT in evaluation of lymph node metastasis in uterine cancer
Abstract
Aim: To investigate diffusion-weighted imaging (DWI) and positron emission tomography and computed tomography (PET/CT) with IV contrast for the preoperative evaluation of pelvic lymph node (LN) metastasis in uterine cancer.
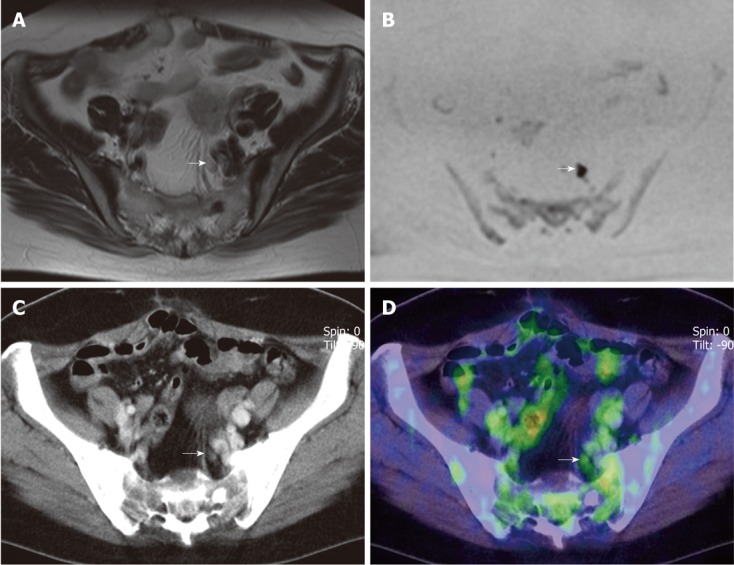
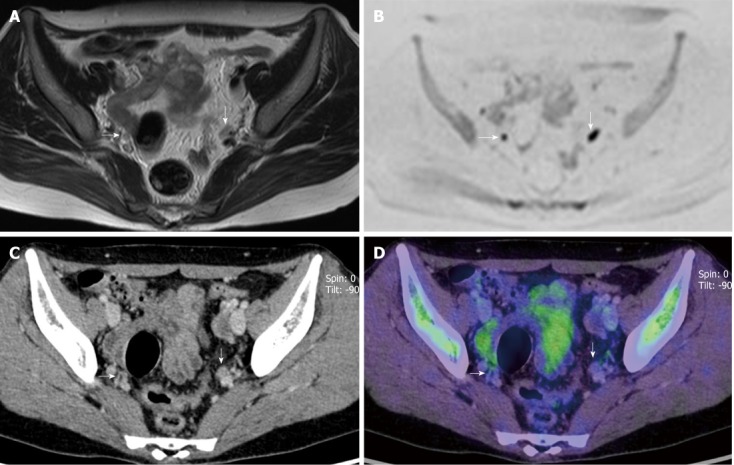
Methods: Twenty-five patients with endometrial or cervical cancer who underwent both DWI and PET/CT before pelvic lymphadenectomy were included in this study. For area specific analysis, LNs were divided into eight regions: both common iliac, external iliac, internal iliac areas, and obturator areas. The classification for malignancy on DWI was a focally abnormal signal intensity in a location that corresponded to the LN chains on the T1WI and T2WI. The criterion for malignancy on PET/CT images was increased tracer uptake by the LN.
Results: A total of 36 pathologically positive LN areas were found in 9 patients. With DWI, the sensitivity, specificity, positive predictive value, negative predictive value and accuracy for detecting metastatic LNs on an LN area-by-area analysis were 83.3%, 51.2%, 27.3%, 93.3% and 57.0%, respectively, while the corresponding values for PET/CT were 38.9%, 96.3%, 70.0%, 87.8% and 86.0%. Differences in sensitivity, specificity and accuracy were significant (P < 0.0005).
Conclusion: DWI showed higher sensitivity and lower specificity than PET/CT. Neither DWI nor PET/CT were sufficiently accurate to replace lymphadenectomy.
Keywords: Diffusion-weighed imaging; Lymph node metastasis; Magnetic resonance imaging; Positron emission tomography and computed tomography; Uterine cancer.
Figures
References
-
- Pecorelli S. Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium. Int J Gynaecol Obstet. 2009;105:103–104. - PubMed
-
- Manetta A, Delgado G, Petrilli E, Hummel S, Barnes W. The significance of paraaortic node status in carcinoma of the cervix and endometrium. Gynecol Oncol. 1986;23:284–290. - PubMed
-
- Creasman WT, Morrow CP, Bundy BN, Homesley HD, Graham JE, Heller PB. Surgical pathologic spread patterns of endometrial cancer. A Gynecologic Oncology Group Study. Cancer. 1987;60:2035–2041. - PubMed
-
- Inoue T, Morita K. The prognostic significance of number of positive nodes in cervical carcinoma stages IB, IIA, and IIB. Cancer. 1990;65:1923–1927. - PubMed
-
- Gal D, Recio FO, Zamurovic D, Tancer ML. Lymphvascular space involvement--a prognostic indicator in endometrial adenocarcinoma. Gynecol Oncol. 1991;42:142–145. - PubMed
LinkOut - more resources
Full Text Sources
