

Cognitive trajectories after postoperative delirium
- PMID: 22762316
- PMCID: PMC3433229
- DOI: 10.1056/NEJMoa1112923
Cognitive trajectories after postoperative delirium
Abstract
Background: Delirium is common after cardiac surgery and may be associated with long-term changes in cognitive function. We examined postoperative delirium and the cognitive trajectory during the first year after cardiac surgery.
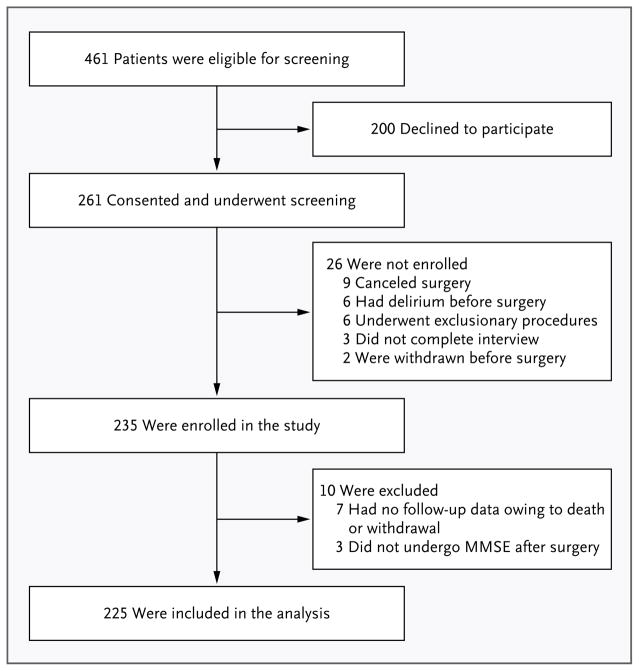
Methods: We enrolled 225 patients 60 years of age or older who were planning to undergo coronary-artery bypass grafting or valve replacement. Patients were assessed preoperatively, daily during hospitalization beginning on postoperative day 2, and at 1, 6, and 12 months after surgery. Cognitive function was assessed with the use of the Mini-Mental State Examination (MMSE; score range, 0 to 30, with lower scores indicating poorer performance). Delirium was diagnosed with the use of the Confusion Assessment Method. We examined performance on the MMSE in the first year after surgery, controlling for demographic characteristics, coexisting conditions, hospital, and surgery type.
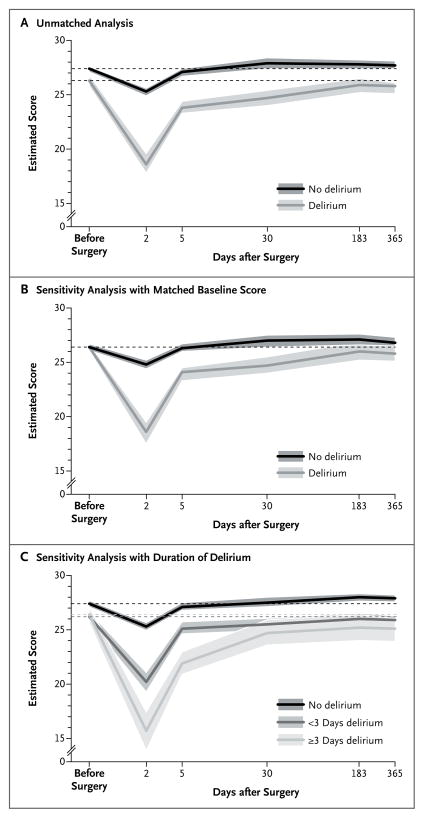
Results: The 103 participants (46%) in whom delirium developed postoperatively had lower preoperative mean MMSE scores than those in whom delirium did not develop (25.8 vs. 26.9, P<0.001). In adjusted models, those with delirium had a larger drop in cognitive function (as measured by the MMSE score) 2 days after surgery than did those without delirium (7.7 points vs. 2.1, P<0.001) and had significantly lower postoperative cognitive function than those without delirium, both at 1 month (mean MMSE score, 24.1 vs. 27.4; P<0.001) and at 1 year (25.2 vs. 27.2, P<0.001) after surgery. With adjustment for baseline differences, the between-group difference in mean MMSE scores was significant 30 days after surgery (P<0.001) but not at 6 or 12 months (P=0.056 for both). A higher percentage of patients with delirium than those without delirium had not returned to their preoperative baseline level at 6 months (40% vs. 24%, P=0.01), but the difference was not significant at 12 months (31% vs. 20%, P=0.055).
Conclusions: Delirium is associated with a significant decline in cognitive ability during the first year after cardiac surgery, with a trajectory characterized by an initial decline and prolonged impairment. (Funded by the Harvard Older Americans Independence Center and others.).
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
Cognitive trajectories after postoperative delirium.N Engl J Med. 2012 Sep 20;367(12):1164; author reply 1164-5. doi: 10.1056/NEJMc1209366. N Engl J Med. 2012. PMID: 22992087 No abstract available.
-
Cognitive trajectories after postoperative delirium.N Engl J Med. 2012 Sep 20;367(12):1164; author reply 1164-5. doi: 10.1056/NEJMc1209366. N Engl J Med. 2012. PMID: 22992088 No abstract available.
References
-
- Raymond PD, Hinton-Bayre AD, Radel M, Ray MJ, Marsh NA. Assessment of statistical change criteria used to define significant change in neuropsychological test performance following cardiac surgery. Eur J Cardiothorac Surg. 2006;29:82–8. - PubMed
-
- Andrew MJ, Baker RA, Bennetts J, Kneebone AC, Knight JL. A comparison of neuropsychologic deficits after extracardiac and intracardiac surgery. J Cardiothorac Vasc Anesth. 2001;15:9–14. - PubMed
-
- Fearn SJ, Pole R, Wesnes K, Faragher EB, Hooper TL, McCollum CN. Cerebral injury during cardiopulmonary bypass: emboli impair memory. J Thorac Cardiovasc Surg. 2001;121:1150–60. - PubMed
-
- Cook DJ, Huston J, III, Trenerry MR, Brown RD, Jr, Zehr KJ, Sundt TM., III Post-cardiac surgical cognitive impairment in the aged using diffusion-weighted magnetic resonance imaging. Ann Thorac Surg. 2007;83:1389–95. - PubMed
-
- Müllges W, Berg D, Schmidtke A, Weinacker B, Toyka KV. Early natural course of transient encephalopathy after coronary artery bypass grafting. Crit Care Med. 2000;28:1808–11. - PubMed
Publication types
MeSH terms
Grants and funding
- P01AG031720/AG/NIA NIH HHS/United States
- P60AG008812/AG/NIA NIH HHS/United States
- K24 AG035075/AG/NIA NIH HHS/United States
- K01AG33643/AG/NIA NIH HHS/United States
- K01 AG033643/AG/NIA NIH HHS/United States
- U01 HL105268/HL/NHLBI NIH HHS/United States
- R01AG030618/AG/NIA NIH HHS/United States
- P01 AG031720/AG/NIA NIH HHS/United States
- P60 AG008812/AG/NIA NIH HHS/United States
- T32 AG023480/AG/NIA NIH HHS/United States
- U01HL105268/HL/NHLBI NIH HHS/United States
- K24AG035075/AG/NIA NIH HHS/United States
- R01 AG030618/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical