

Effect of adding a diagnostic aid to best practice to manage suspicious pigmented lesions in primary care: randomised controlled trial
- PMID: 22763392
- PMCID: PMC3389518
- DOI: 10.1136/bmj.e4110
Effect of adding a diagnostic aid to best practice to manage suspicious pigmented lesions in primary care: randomised controlled trial
Abstract
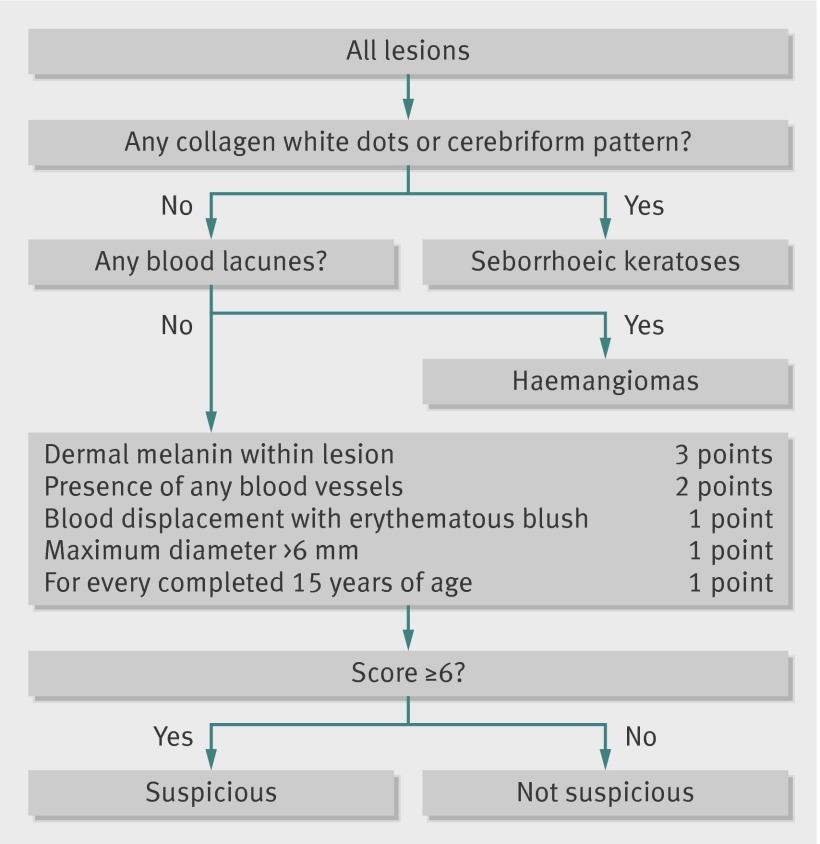
Objectives: To assess whether adding a novel computerised diagnostic tool, the MoleMate system (SIAscopy with primary care scoring algorithm), to current best practice results in more appropriate referrals of suspicious pigmented lesions to secondary care, and to assess its impact on clinicians and patients.
Design: Randomised controlled trial.
Setting: 15 general practices in eastern England.
Participants: 1297 adults with pigmented skin lesions not immediately diagnosed as benign.
Interventions: Patients were assessed by trained primary care clinicians using best practice (clinical history, naked eye examination, seven point checklist) either alone (control group) or with the MoleMate system (intervention group).
Main outcome measures: Appropriateness of referral, defined as the proportion of referred lesions that were biopsied or monitored. Secondary outcomes related to the clinicians (diagnostic performance, confidence, learning effects) and patients (satisfaction, anxiety). Economic evaluation, diagnostic performance of the seven point checklist, and five year follow-up of melanoma incidence were also secondary outcomes and will be reported later.
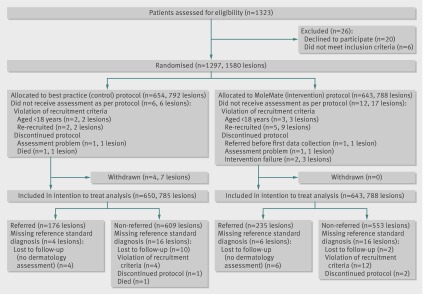
Results: 1297 participants with 1580 lesions were randomised: 643 participants with 788 lesions to the intervention group and 654 participants with 792 lesions to the control group. The appropriateness of referral did not differ significantly between the intervention or control groups: 56.8% (130/229) v 64.5% (111/172); difference -8.1% (95% confidence interval -18.0% to 1.8%). The proportion of benign lesions appropriately managed in primary care did not differ (intervention 99.6% v control 99.2%, P=0.46), neither did the percentage agreement with an expert decision to biopsy or monitor (intervention 98.5% v control 95.7%, P=0.26). The percentage agreement with expert assessment that the lesion was benign was significantly lower with MoleMate (intervention 84.4% v control 90.6%, P<0.001), and a higher proportion of lesions were referred (intervention 29.8% v control 22.4%, P=0.001). Thirty six histologically confirmed melanomas were diagnosed: 18/18 were appropriately referred in the intervention group and 17/18 in the control group. Clinicians in both groups were confident, and there was no evidence of learning effects, and therefore contamination, between groups. Patients in the intervention group ranked their consultations higher for thoroughness and reassuring care, although anxiety scores were similar between the groups.
Conclusions: We found no evidence that the MoleMate system improved appropriateness of referral. The systematic application of best practice guidelines alone was more accurate than the MoleMate system, and both performed better than reports of current practice. Therefore the systematic application of best practice guidelines (including the seven point checklist) should be the paradigm for management of suspicious skin lesions in primary care.
Trial registration: Current Controlled Trials ISRCTN79932379.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures

Comment in
-
Identifying melanomas in primary care: can we do better?BMJ. 2012 Jul 4;345:e4244. doi: 10.1136/bmj.e4244. BMJ. 2012. PMID: 22763394 No abstract available.
References
-
- Murchie P, Campbell NC. Pigmented lesions, cutaneous melanoma, and future challenges for primary care. Eur J Gen Pract 2007;13:151-4. - PubMed
-
- Lens MB, Dawes M. Global perspectives of contemporary epidemiological trends of cutaneous malignant melanoma. Br J Dermatol 2004;150:179-85. - PubMed
-
- All-Party Parliamentary Group on Skin. Report on the enquiry into the treatment, management and prevention of skin cancer. All-Party Parliamentary Group on Skin, 2003.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical