

Review
doi: 10.1177/0883073812448231.
Epub 2012 Jul 4.
Childhood cerebellar ataxia
Affiliations
- PMID: 22764177
- PMCID: PMC3490706
- DOI: 10.1177/0883073812448231
Item in Clipboard
Review
Childhood cerebellar ataxia
J Child Neurol.
2012 Sep.
Abstract
Childhood presentations of ataxia, an impairment of balance and coordination caused by damage to or dysfunction of the cerebellum, can often be challenging to diagnose. Presentations tend to be clinically heterogeneous, but key considerations may vary based on the child's age at onset, the course of illness, and subtle differences in phenotype. Systematic investigation is recommended for efficient diagnosis. In this review, we outline common etiologies and describe a comprehensive approach to the evaluation of both acquired and genetic cerebellar ataxia in children.
Figures
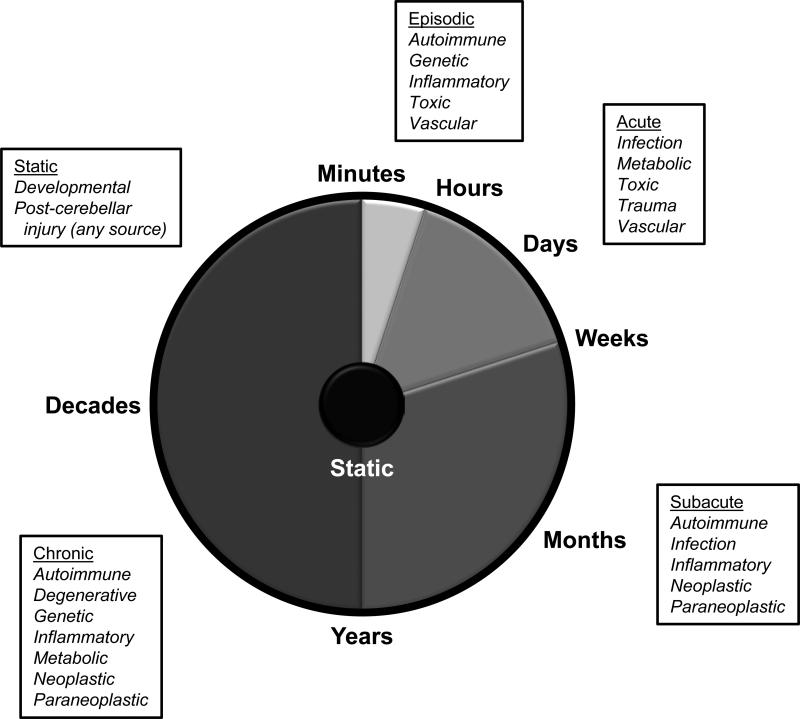
Differential diagnosis of ataxia for given rates of disease progression. Various tempos of cerebellar disease are shown with common etiologies for consideration indicated.
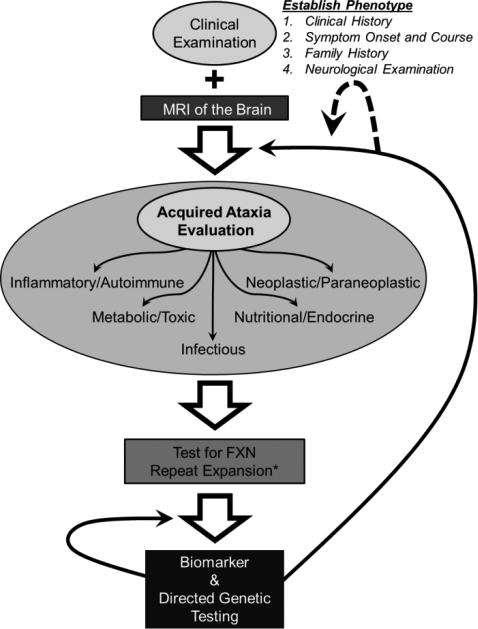
Evaluation of the child with cerebellar ataxia. All patients require a through clinical examination to establish the phenotype of their disease. This includes a complete history of illness with onset of symptoms and detailed course, family history, and neurological examination. MRI of the brain can provide additional detail as well as identify certain vascular, developmental, traumatic, and neoplastic etiologies, among others. A detailed evaluation of acquired causes, particularly those amenable to treatment, follows. Such evaluation should be targeted to etiologies suggested from the clinical examination. If a genetic etiology is suspected, all patients should be tested for repeat expansion in the frataxin (FXN) gene. FXN sequencing for point mutations should only be performed in patients with an identified expansion on one allele (*). If normal, biomarker screening should be performed and, if negative, followed by genetic testing directed toward the identified phenotype. If unsuccessful, re-evaluation can include additional genetic or acquired testing (black arrows), particularly if new symptoms arise, prompting a re-definition of the patient's phenotype (dashed arrow).

Neuroimaging in acquired and genetic cerebellar ataxia and diagnostic mislabeling. Sagittal T1-weighted MRI of the cervical spine and posterior fossa is shown for 3 adolescent patients. (A) Unaffected individual showing normal cerebellar vermis and cervical spinal cord. (B) A patient with genetically-proven autosomal recessive spastic ataxia of Charlevoix-Saguenay (ARSACS), demonstrating atrophy of the midline cerebellar vermis and thinning of the cervical spinal cord (arrows). This patient presented having carried a diagnosis of cerebral palsy throughout her entire childhood. (C) A patient with autoimmune-mediated ataxia showing midline cerebellar vermian atrophy (arrow). This patient presented with a clinical diagnosis of Friedreich ataxia despite acute and severe symptom onset and had a subsequently negative gene test . Acquired workup showed mild elevations of several autoantibodies but was otherwise unremarkable, so the patient was given an empiric course of steroids, resulting in stabilization of symptoms over the following year.
References
-
- Fogel BL, Perlman S. Cerebellar disorders: Balancing the approach to cerebellar ataxia. In: Gálvez-Jiménez N, Tuite PJ, editors. Uncommon Causes of Movement Disorders. 1st ed Cambridge University Press; 2011. pp. 198–216.
-
- Fogel BL, Perlman S. An approach to the patient with late-onset cerebellar ataxia. Nat Clin Pract Neurol. 2006;2:629–635. quiz 1 p following 635. - PubMed
-
- Klockgether T. Sporadic ataxia with adult onset: classification and diagnostic criteria. Lancet Neurol. 2010;9:94–104. - PubMed
-
- Brusse E, Maat-Kievit JA, van Swieten JC. Diagnosis and management of early-and late-onset cerebellar ataxia. Clin Genet. 2007;71:12–24. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
