

The BOLERO-2 trial: the addition of everolimus to exemestane in the treatment of postmenopausal hormone receptor-positive advanced breast cancer
- PMID: 22764762
- PMCID: PMC3466807
- DOI: 10.2217/fon.12.49
The BOLERO-2 trial: the addition of everolimus to exemestane in the treatment of postmenopausal hormone receptor-positive advanced breast cancer
Abstract
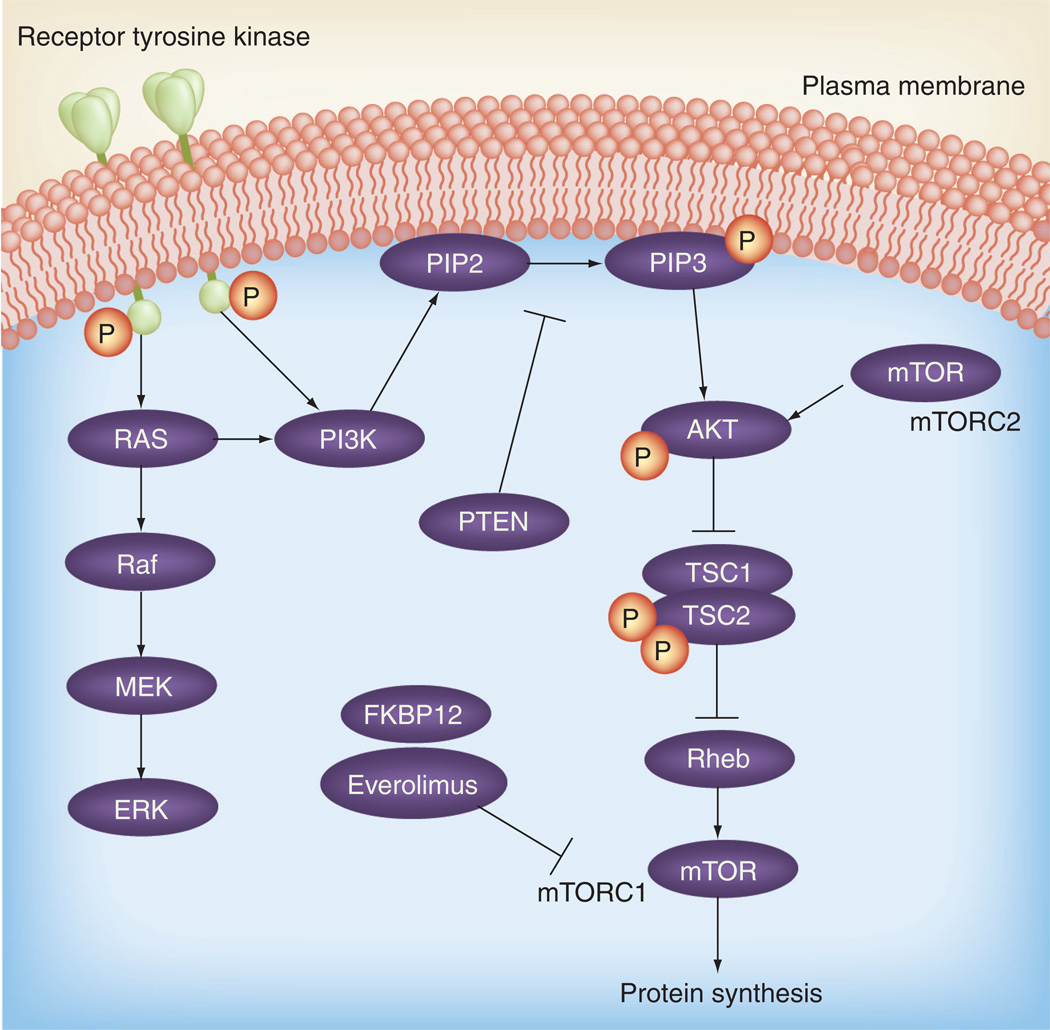
The combination of the mTOR inhibitor everolimus with the aromatase inhibitor exemestane was evaluated in the randomized Phase III BOLERO-2 trial. Research has indicated that aberrant signaling through the mTOR pathway is associated with resistance to endocrine therapies. The BOLERO-2 trial examined the effects on progression-free survival of the addition of everolimus to exemestane in a patient population of postmenopausal, hormone receptor-positive, advanced breast cancer. At the interim analysis, the median progression-free survival assessed by local investigators was 6.9 months for everolimus plus exemestane versus 2.8 months for placebo plus exemestane (hazard ratio: 0.43; p < 0.001), and by central assessment was 10.6 versus 4.1 months, respectively (hazard ratio: 0.36; p < 0.001). The everolimus plus exemestane arm showed greater number of grade 3 and 4 adverse events. This study suggests that the addition of everolimus to exemestane is a potential viable treatment option for this patient population.
Conflict of interest statement
The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Figures
References
-
- Ali S, Coombes RC. Endocrine-responsive breast cancer and strategies for combating resistance. Nat. Rev. Cancer. 2002;2(2):101–112. - PubMed
-
- Smith IE, Dowsett M. Aromatase inhibitors in breast cancer. N. Engl. J. Med. 2003;348(24):2431–2442. - PubMed
-
- Mouridsen H, Sun Y, Gershanovich M, et al. Superiority of letrozole to tamoxifen in the first-line treatment of advanced breast cancer: evidence from metastatic subgroups and a test of functional ability. Oncologist. 2004;9(5):489–496. - PubMed
-
- Nabholtz JM, Buzdar A, Pollak M, et al. Anastrozole is superior to tamoxifen as first-line therapy for advanced breast cancer in postmenopausal women: results of a North American multicenter randomized trial. Arimidex Study Group. J. Clin. Oncol. 2000;18(22):3758–3767. - PubMed
-
- Bonneterre J, Thurlimann B, Robertson JF, et al. Anastrozole versus tamoxifen as first-line therapy for advanced breast cancer in 668 postmenopausal women: results of the Tamoxifen or Arimidex Randomized Group Efficacy and Tolerability study. J. Clin. Oncol. 2000;18(22):3748–3757. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous