

Semi-automated vectorial analysis of anorectal motion by magnetic resonance defecography in healthy subjects and fecal incontinence
- PMID: 22765510
- PMCID: PMC3440517
- DOI: 10.1111/j.1365-2982.2012.01962.x
Semi-automated vectorial analysis of anorectal motion by magnetic resonance defecography in healthy subjects and fecal incontinence
Abstract
Background: Inter-observer variability limits the reproducibility of pelvic floor motion measured by magnetic resonance imaging (MRI). Our aim was to develop a semi-automated program measuring pelvic floor motion in a reproducible and refined manner.
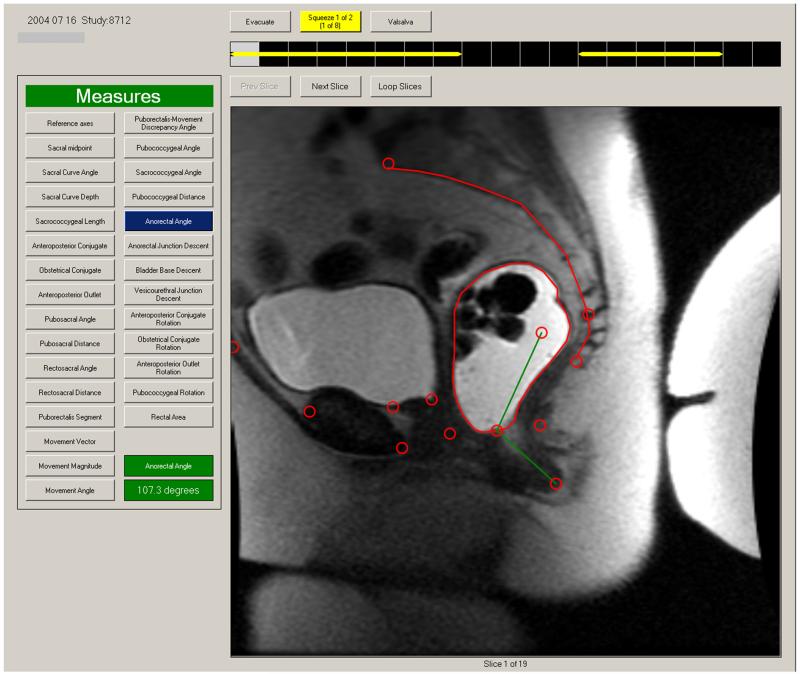
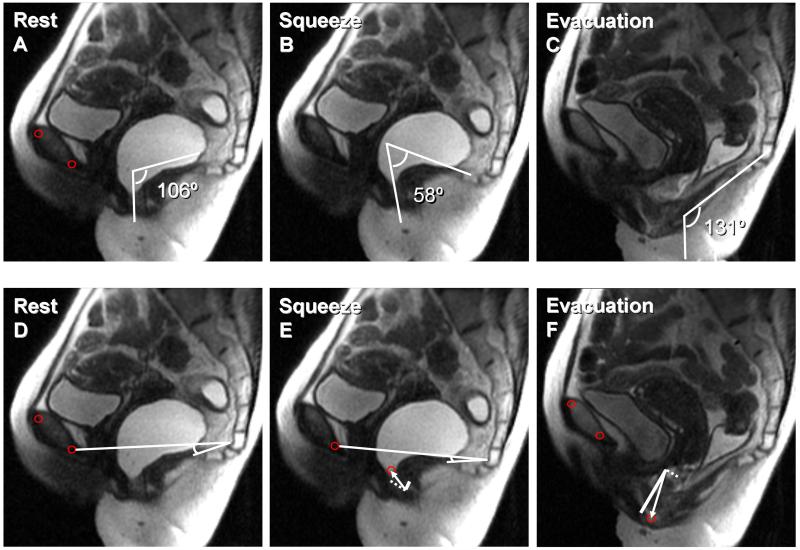
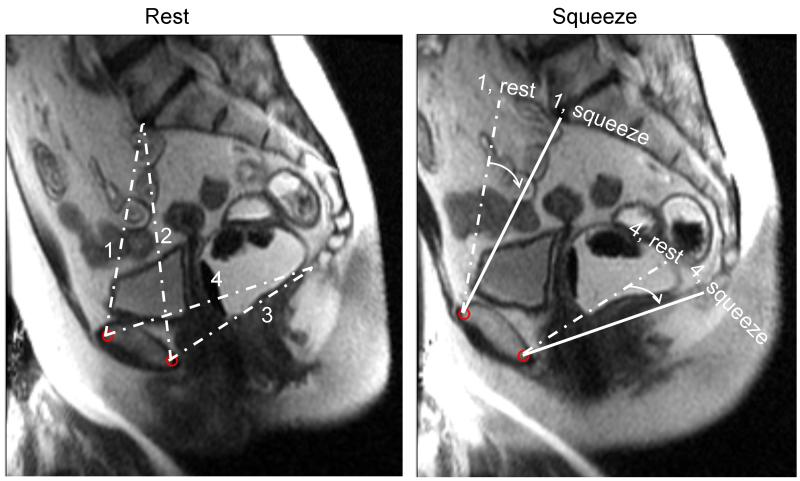
Methods: Pelvic floor anatomy and motion during voluntary contraction (squeeze) and rectal evacuation were assessed by MRI in 64 women with fecal incontinence (FI) and 64 age-matched controls. A radiologist measured anorectal angles and anorectal junction motion. A semi-automated program did the same and also dissected anorectal motion into perpendicular vectors representing the puborectalis and other pelvic floor muscles, assessed the pubococcygeal angle, and evaluated pelvic rotation.
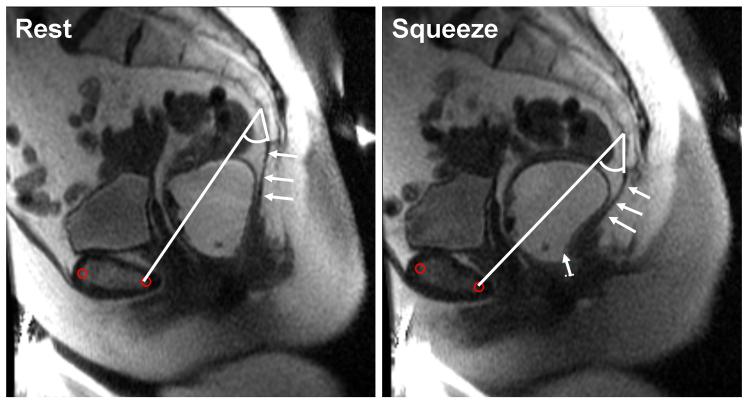
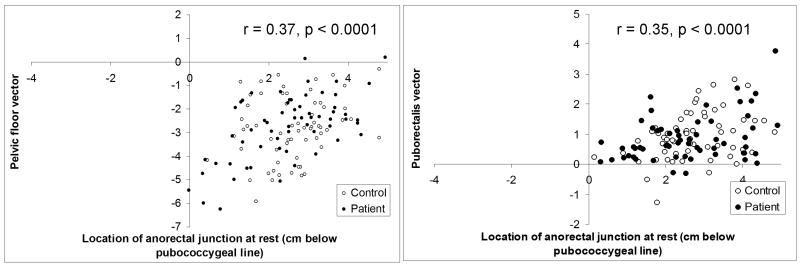
Key results: Manual and semi-automated measurements of anorectal junction motion (r = 0.70; P < 0.0001) during squeeze and evacuation were correlated, as were anorectal angles at rest, squeeze, and evacuation; angle change during squeeze or evacuation was less so. Semi-automated measurements of anorectal and pelvic bony motion were also reproducible within subjects. During squeeze, puborectalis injury was associated (P ≤ 0.01) with smaller puborectalis but not pelvic floor motion vectors, reflecting impaired puborectalis function. The pubococcygeal angle, reflecting posterior pelvic floor motion, was smaller during squeeze and larger during evacuation. However, pubococcygeal angles and pelvic rotation during squeeze and evacuation did not differ significantly between FI and controls.
Conclusion & inferences: This semi-automated program provides a reproducible, efficient, and refined analysis of pelvic floor motion by MRI. Puborectalis injury is independently associated with impaired motion of puborectalis, not other pelvic floor muscles in controls and women with FI.
© 2012 Blackwell Publishing Ltd.
Figures
References
-
- Bharucha AE. Pelvic floor: anatomy and function. Neurogastroenterology & Motility. 2006;18:507–519. - PubMed
-
- Diamant NE, Kamm MA, Wald A, Whitehead WE. American Gastroenterological Association Medical Position Statement on Anorectal Testing Techniques. Gastroenterology. 1999;116:732–760. - PubMed
-
- Bharucha AE, Wald A, Enck P, Rao S. Functional anorectal disorders. Gastroenterology. 2006;130:1510–1518. - PubMed
-
- Bharucha AE. Update of tests of colon and rectal structure and function. Journal of Clinical Gastroenterology. 2006;40:96–103. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
