

MRI evidence of impaired CSF homeostasis in obesity-associated idiopathic intracranial hypertension
- PMID: 22766676
- PMCID: PMC7966351
- DOI: 10.3174/ajnr.A3171
MRI evidence of impaired CSF homeostasis in obesity-associated idiopathic intracranial hypertension
Abstract
Background and purpose: Impaired CSF homeostasis and altered venous hemodynamics are proposed mechanisms for elevated pressure in IIH. However, the lack of ventricular expansion steered the focus away from CSF homeostasis in IIH. This study aims to measure intracranial CSF volumes and cerebral venous drainage with MR imaging to determine whether increased CSF volume from impaired CSF homeostasis and venous hemodynamics occur in obesity-related IIH.
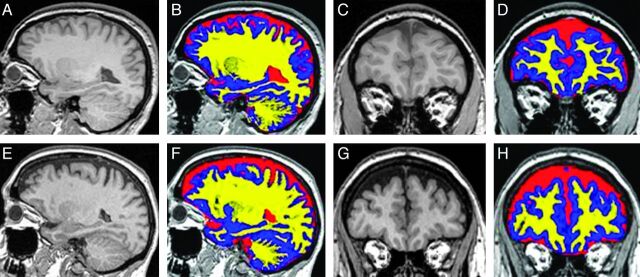
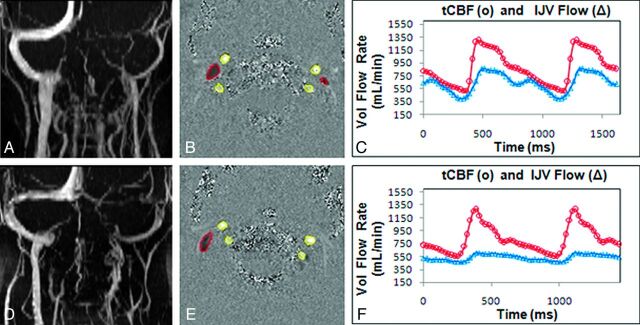
Materials and methods: Two homogeneous cohorts of 11 newly diagnosed pretreatment overweight women with IIH and 11 overweight healthy women were prospectively studied. 3D volumetric MR imaging of the brain was used to quantify CSF and brain tissue volumes, and dynamic phase contrast was used to measure relative cerebral drainage through the internal jugular veins.
Results: Findings confirm normal ventricular volume in IIH. However, extraventricular CSF volume is significantly increased in IIH (290 ± 52 versus 220 ± 24 mL, P = .001). This is even more significant after normalization with intracranial volume (P = .0007). GM interstitial fluid volume is also increased in IIH (602 ± 57 versus 557 ± 31 mL, P = .037). Total arterial inflow is normal, but relative venous drainage through the IJV is significantly reduced in IIH (65 ± 7% versus 81 ± 10%, P = .001).
Conclusions: Increased intracranial CSF volume that accumulates in the extraventricular subarachnoid space provides direct evidence for impaired CSF homeostasis in obesity-associated IIH. The finding of larger GM interstitial fluid volume is consistent with increased overall resistance to cerebral venous drainage, as evident from reduced relative cerebral drainage through the IJV. The present study confirms that both impaired CSF homeostasis and venous hemodynamics coexist in obesity-associated IIH.
Figures
References
-
- Wall M, George D. Idiopathic intracranial hypertension. Brain 1991;114:155–80 - PubMed
-
- Friesner D, Rosenman R, Lobb BM, et al. . Idiopathic intracranial hypertension in the USA: the role of obesity in establishing prevalence and healthcare costs. Obes Rev 2010;12:1–8 - PubMed
-
- Pearce JM. From pseudotumour cerebri to idiopathic intracranial hypertension. Pract Neurol 2009;9:353–56 - PubMed
-
- Alperin N, Lee SH, Mazda M, et al. . Evidence for the importance of extracranial venous flow in patients with idiopathic intracranial hypertension (IIH). Acta Neurochir Suppl 2005;95:129–32 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical