

Meta-analysis of efficacy of interventions for elevated depressive symptoms in adults diagnosed with cancer
- PMID: 22767203
- PMCID: PMC3634552
- DOI: 10.1093/jnci/djs256
Meta-analysis of efficacy of interventions for elevated depressive symptoms in adults diagnosed with cancer
Abstract
Background: Cancer patients are at increased risk for depression compared with individuals with no cancer diagnosis, yet few interventions target depressed cancer patients.
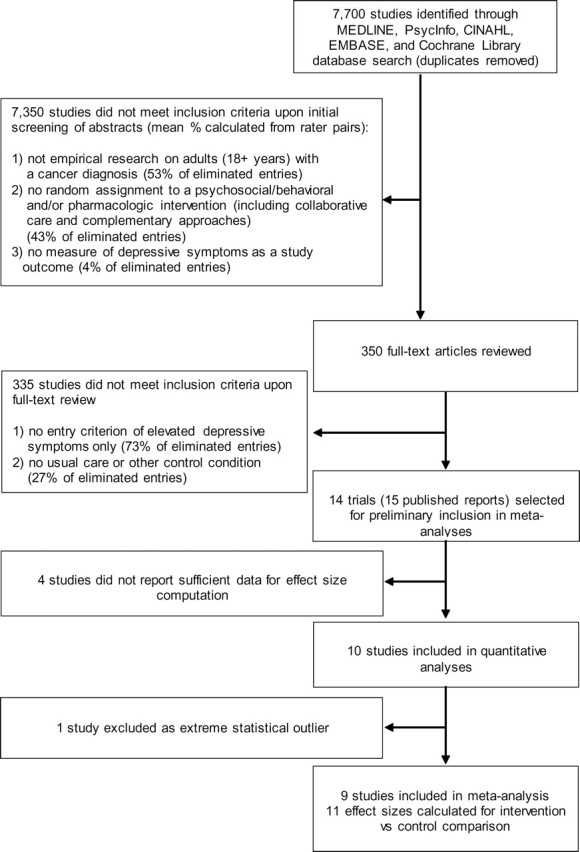
Methods: Efficacy of psychotherapeutic and pharmacologic interventions for depression in cancer patients who met an entry threshold for depressive symptoms was examined by meta-analysis. Five electronic databases were systematically reviewed to identify randomized controlled trials meeting the selection criteria. Effect sizes were calculated using Hedges' g and were pooled to compare pre- and postrandomization depressive symptoms with a random effects model. Subgroup analyses tested moderators of effect sizes, such as comparison of different intervention modalities, with a mixed effects model. All statistical tests were two-sided.
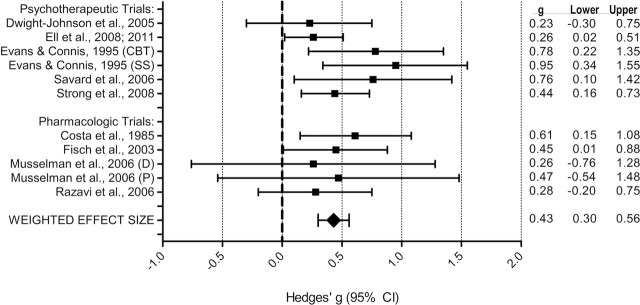
Results: Ten randomized controlled trials (six psychotherapeutic and four pharmacologic studies) met the selection criteria; 1362 participants with mixed cancer types and stages had been randomly assigned to treatment groups. One outlier trial was removed from analyses. The random effects model showed interventions to be superior to control conditions on reducing depressive symptoms postintervention (Hedges' g = 0.43, 95% confidence interval = 0.30 to 0.56, P < .001). In the four psychotherapeutic trials with follow-up assessment, interventions were more effective than control conditions up to 12-18 months after patients were randomly assigned to treatment groups (P < .001). Although each approach was more effective than the control conditions in improving depressive symptoms (P < .001), subgroup analyses showed that cognitive behavioral therapy appeared more effective than problem-solving therapy (P = .01), but not more effective than pharmacologic intervention (P = .07).
Conclusions: Our findings suggest that psychological and pharmacologic approaches can be targeted productively toward cancer patients with elevated depressive symptoms. Research is needed to maximize effectiveness, accessibility, and integration into clinical care of interventions for depressed cancer patients.
Figures
Comment in
-
Re: Meta-analysis of efficacy of interventions elevated depressive symptoms in adults diagnosed with cancer.J Natl Cancer Inst. 2012 Nov 21;104(22):1770; author reply 1770-1. doi: 10.1093/jnci/djs408. Epub 2012 Sep 21. J Natl Cancer Inst. 2012. PMID: 23000656 No abstract available.
References
-
- Polsky D, Doshi JA, Marcus S, et al. Long-term risk for depressive symptoms after a medical diagnosis Arch Intern Med 2005;165 11):1260 1266 - PubMed
-
- Mitchell AJ, Chan M, Bhatti H, et al. Prevalence of depression, anxiety, and adjustment disorder in oncological, haematological, and palliative-care settings: a meta-analysis of 94 interview-based studies Lancet Oncol 2011;12 2):160 174 - PubMed
-
- DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor for noncompliance with medical treatment: meta-analysis of the effects of anxiety and depression on patient adherence Arch Intern Med 2000;160 14):2101 2107 - PubMed
-
- Himelhoch S, Weller WE, Wu AW, et al. Chronic medical illness, depression, and use of acute medical services among Medicare beneficiaries Med Care 2004;42 6):512 521 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
