

Patient treatment preference as a predictor of response and attrition in treatment for chronic depression
- PMID: 22767424
- PMCID: PMC3463778
- DOI: 10.1002/da.21977
Patient treatment preference as a predictor of response and attrition in treatment for chronic depression
Abstract
Background: Findings regarding the relationship between patient treatment preference and treatment outcome are mixed. This is a secondary data analysis investigating the relationship between treatment preference, and symptom outcome and attrition in a large two-phase depression treatment trial.
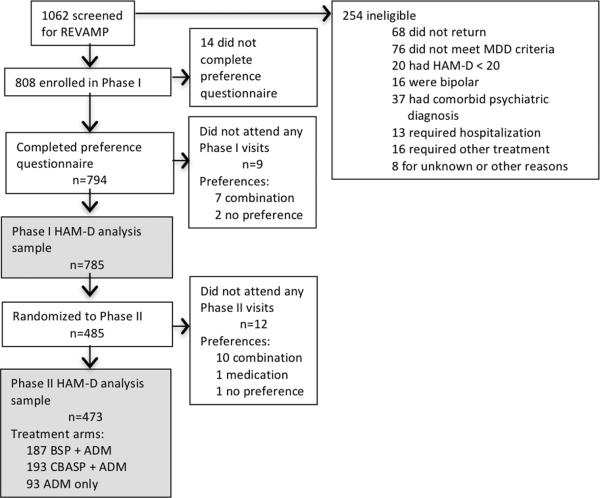
Methods: Patients met DSM-IV criteria for chronic forms of depression. Phase I was a 12-week, nonrandomized, open-label trial in which all participants (n = 785) received antidepressant medication(s) (ADM). Phase I nonremitters were randomized to Phase II, in which they received 12 weeks of either cognitive-behavioral system of psychotherapy (CBASP) + ADM (n = 193), brief supportive psychotherapy (BSP) + ADM (n = 187), or ADM only (n = 93). Participants indicated their treatment preference (medication only, combined treatment or no preference) at study entry. Symptoms were measured at 2-week intervals with the 24-item Hamilton Rating Scale for Depression (HAM-D).
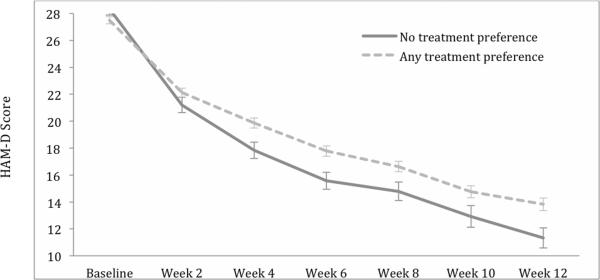
Results: A large majority of patients reported a preference for combined treatment. Patients who preferred medication only were more likely to endorse a chemical imbalance explanation for depression, whereas those desiring combined treatment were more likely to attribute their depression to stressful experiences. In Phase I, patients who expressed no treatment preference showed greater rates of HAM-D symptom reduction than those with any preference, and patients with a preference for medication showed higher attrition than those preferring combined treatment. In Phase II, baseline treatment preference was not associated with symptom reduction or attrition.
Conclusions: Treatment preferences may moderate treatment response and attrition in unexpected ways. Research identifying factors associated with differing preferences may enable improved treatment retention and response.
© 2012 Wiley Periodicals, Inc.
Figures
Similar articles
-
Cognitive behavioral analysis system of psychotherapy and brief supportive psychotherapy for augmentation of antidepressant nonresponse in chronic depression: the REVAMP Trial.Arch Gen Psychiatry. 2009 Nov;66(11):1178-88. doi: 10.1001/archgenpsychiatry.2009.144. Arch Gen Psychiatry. 2009. PMID: 19884606 Free PMC article. Clinical Trial.
-
The relationship between the therapeutic alliance and treatment outcome in two distinct psychotherapies for chronic depression.J Consult Clin Psychol. 2013 Aug;81(4):627-38. doi: 10.1037/a0031530. Epub 2013 Jan 21. J Consult Clin Psychol. 2013. PMID: 23339536 Free PMC article. Clinical Trial.
-
The influence of patients' preference/attitude towards psychotherapy and antidepressant medication on the treatment of major depressive disorder.J Behav Ther Exp Psychiatry. 2014 Mar;45(1):170-7. doi: 10.1016/j.jbtep.2013.10.003. Epub 2013 Oct 15. J Behav Ther Exp Psychiatry. 2014. PMID: 24172145 Clinical Trial.
-
Novel Augmentation Strategies in Major Depression.Dan Med J. 2017 Apr;64(4):B5338. Dan Med J. 2017. PMID: 28385173 Review.
-
Psychotherapy or medication for depression? Using individual symptom meta-analyses to derive a Symptom-Oriented Therapy (SOrT) metric for a personalised psychiatry.BMC Med. 2020 Jun 5;18(1):170. doi: 10.1186/s12916-020-01623-9. BMC Med. 2020. PMID: 32498707 Free PMC article.
Cited by
-
The effects of amount of home meditation practice in Mindfulness Based Cognitive Therapy on hazard of relapse to depression in the Staying Well after Depression Trial.Behav Res Ther. 2014 Dec;63:17-24. doi: 10.1016/j.brat.2014.08.015. Epub 2014 Aug 30. Behav Res Ther. 2014. PMID: 25261599 Free PMC article. Clinical Trial.
-
Effectiveness of a decision aid for patients with depression: A randomized controlled trial.Health Expect. 2017 Oct;20(5):1096-1105. doi: 10.1111/hex.12553. Epub 2017 Mar 10. Health Expect. 2017. PMID: 28295915 Free PMC article. Clinical Trial.
-
Cognitive-Behavioural Analysis System of Psychotherapy (CBASP), a drug, or their combination: differential therapeutics for persistent depressive disorder: a study protocol of an individual participant data network meta-analysis.BMJ Open. 2016 May 4;6(5):e011769. doi: 10.1136/bmjopen-2016-011769. BMJ Open. 2016. PMID: 27147393 Free PMC article.
-
Prescriptive Predictors of Mindfulness Ecological Momentary Intervention for Social Anxiety Disorder: Machine Learning Analysis of Randomized Controlled Trial Data.JMIR Ment Health. 2025 May 13;12:e67210. doi: 10.2196/67210. JMIR Ment Health. 2025. PMID: 40359509 Free PMC article. Clinical Trial.
-
Ketamine treatment for depression: qualitative study exploring patient views.BJPsych Open. 2021 Jan 11;7(1):e32. doi: 10.1192/bjo.2020.165. BJPsych Open. 2021. PMID: 33427156 Free PMC article.
References
-
- World Health Organiziation . Depression Management Fact Sheet. 2011.
-
- Kessler RC, Berglund P, Demler O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593–602. - PubMed
-
- Swift JK, Callahan JL, Vollmer BM. Preferences. J Clin Psychol. 2011;67(2):155–65. - PubMed
-
- van Schaik DJ, Klijn AF, van Hout HP, et al. Patients' preferences in the treatment of depressive disorder in primary care. General hospital psychiatry. 2004;26(3):184–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- UO1 MH61590/MH/NIMH NIH HHS/United States
- T32 MH019938/MH/NIMH NIH HHS/United States
- U01 MH061562/MH/NIMH NIH HHS/United States
- UO1 MH62475/MH/NIMH NIH HHS/United States
- U01 MH062475/MH/NIMH NIH HHS/United States
- U01 MH061590/MH/NIMH NIH HHS/United States
- UO1 MH61587/MH/NIMH NIH HHS/United States
- UO1 MH61504/MH/NIMH NIH HHS/United States
- U01 MH062546/MH/NIMH NIH HHS/United States
- U01 MH061504/MH/NIMH NIH HHS/United States
- UO1 MH62546/MH/NIMH NIH HHS/United States
- U01 MH62491/MH/NIMH NIH HHS/United States
- U01 MH062491/MH/NIMH NIH HHS/United States
- 5T32MH019938-18/MH/NIMH NIH HHS/United States
- U01 MH063481/MH/NIMH NIH HHS/United States
- U01 MH062465/MH/NIMH NIH HHS/United States
- U01 MH061587/MH/NIMH NIH HHS/United States
- U01 MH62465/MH/NIMH NIH HHS/United States
- UO1 MH61562/MH/NIMH NIH HHS/United States
- UO1 MH63481/MH/NIMH NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
