

Lessons on Tumour Response: Imaging during Therapy with (177)Lu-DOTA-octreotate. A Case Report on a Patient with a Large Volume of Poorly Differentiated Neuroendocrine Carcinoma
- PMID: 22768026
- PMCID: PMC3360199
- DOI: 10.7150/thno.3594
Lessons on Tumour Response: Imaging during Therapy with (177)Lu-DOTA-octreotate. A Case Report on a Patient with a Large Volume of Poorly Differentiated Neuroendocrine Carcinoma
Abstract
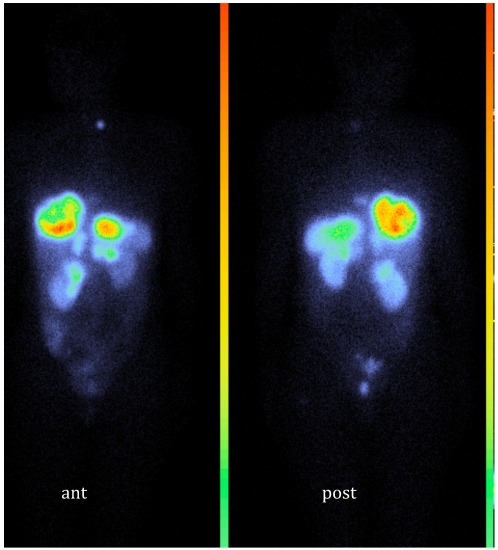
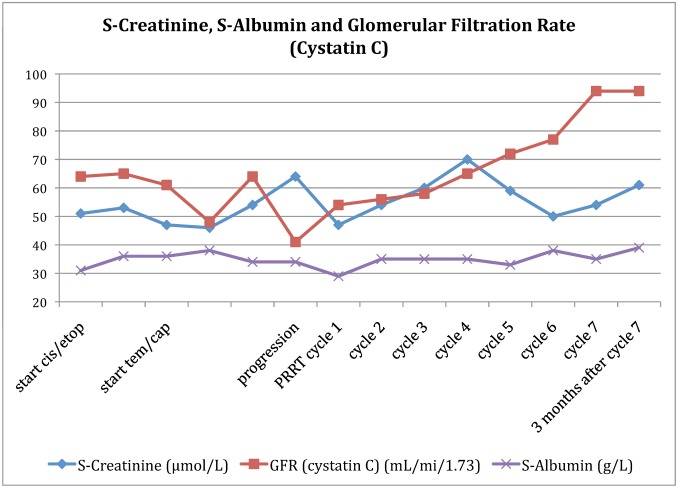
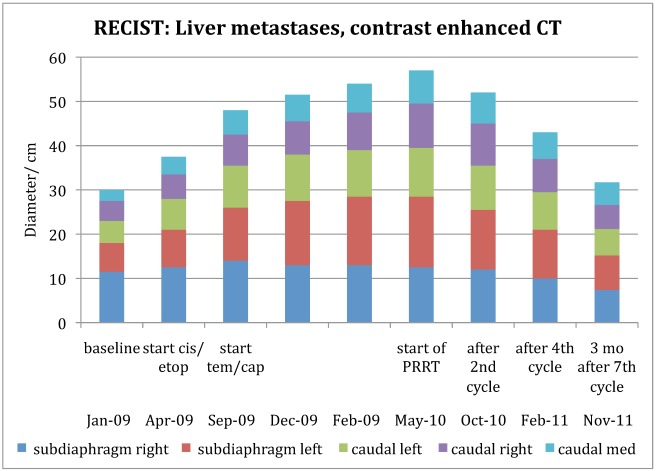
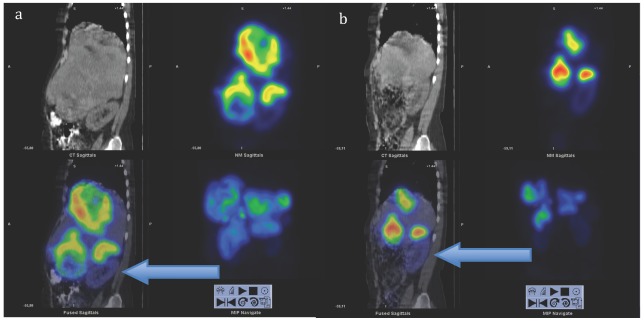
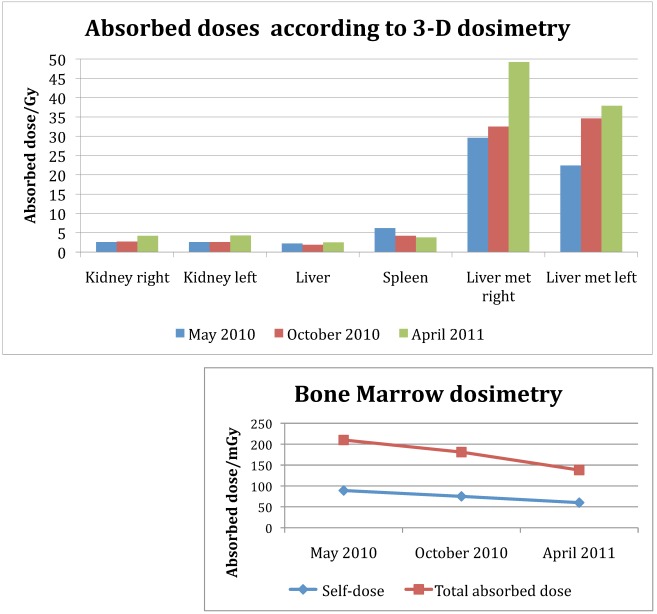
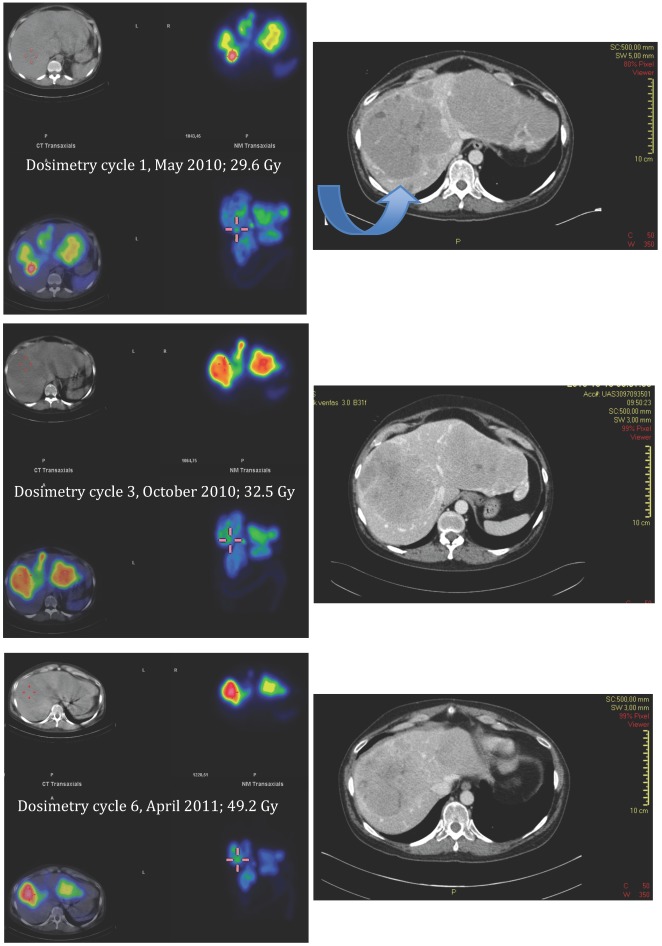
Favourable outcomes of peptide receptor radiotherapy (PRRT) of neuroendocrine tumours have been reported during the last years. Still, there are uncertainties on the radionuclides to be used, the treatment planning, and the indication in patients with a high proliferation rate.This case report describes a patient with a high tumour burden of poorly differentiated neuroendocrine carcinoma of unknown primary with a proliferation rate in liver metastases up to 50%, undergoing fractionated treatment with 7 cycles of (177)Lu-DOTA-octreotate (7.4 GBq each) after disease progression on two different chemotherapy regiments. Based on initial staging scintigraphy, somatostatin receptor expression was very high.Longitudinal dosimetry studies during therapy indicated ongoing increases in tumour-to-organ ratios that coincided with an objective response.We conclude that fractionated therapy with (177)Lu-DOTA-octreotate should be considered a treatment option also for those patients with large tumours, high proliferation, and high receptor expression.
Keywords: 177Lu-DOTA-octreotate; Neuroendocrine tumour; PRRT; dosimetry.; radionuclide therapy.
Conflict of interest statement
Competing Interests: The authors have declared that no competing interest exists.
Figures



References
-
- Imhof A, Brunner P, Marincek N, Briel M, Schindler C, Rasch H, Macke HR, Rochlitz C, Muller-Brand J, Walter MA. Response, survival, and long-term toxicity after therapy with the radiolabeled somatostatin analogue [90Y-DOTA]-TOC in metastasized neuroendocrine cancers. J Clin Oncol. 2011;29(17):2416–23. - PubMed
-
- Kwekkeboom DJ, Teunissen JJ, Bakker WH, Kooij PP, de Herder WW, Feelders RA, van Eijck CH, Esser JP, Kam BL, Krenning EP. Radiolabeled somatostatin analog [177Lu-DOTA0,Tyr3]octreotate in patients with endocrine gastroenteropancreatic tumors. J Clin Oncol. 2005;23(12):2754–62. - PubMed
-
- Kwekkeboom DJ, de Herder WW, Kam BL, van Eijck CH, van Essen M, Kooij PP, Feelders RA, van Aken MO, Krenning EP. Treatment with the radiolabeled somatostatin analog [177 Lu-DOTA 0,Tyr3]octreotate: toxicity, efficacy, and survival. J Clin Oncol. 2008;26(13):2124–30. - PubMed
-
- Hoefnagel CA. Metaiodobenzylguanidine and somatostatin in oncology: role in the management of neural crest tumours. Eur J Nucl Med. 1994;21(6):561–81. - PubMed
-
- Hoefnagel CA, De Kraker J, Valdes Olmos RA, Voute PA. 131I-MIBG as a first-line treatment in high-risk neuroblastoma patients. Nucl Med Commun. 1994;15(9):712–7. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
