

Fact or factitious? A psychobiological study of authentic and simulated dissociative identity states
- PMID: 22768068
- PMCID: PMC3387157
- DOI: 10.1371/journal.pone.0039279
Fact or factitious? A psychobiological study of authentic and simulated dissociative identity states
Erratum in
- PLoS One. 2012;7(7): doi/10.1371/annotation/4f2000ce-ff9e-48e8-8de0-893b67efa3a4. Reinders, A A T Simone [corrected to Reinders, A A T S].
Abstract
Background: Dissociative identity disorder (DID) is a disputed psychiatric disorder. Research findings and clinical observations suggest that DID involves an authentic mental disorder related to factors such as traumatization and disrupted attachment. A competing view indicates that DID is due to fantasy proneness, suggestibility, suggestion, and role-playing. Here we examine whether dissociative identity state-dependent psychobiological features in DID can be induced in high or low fantasy prone individuals by instructed and motivated role-playing, and suggestion.
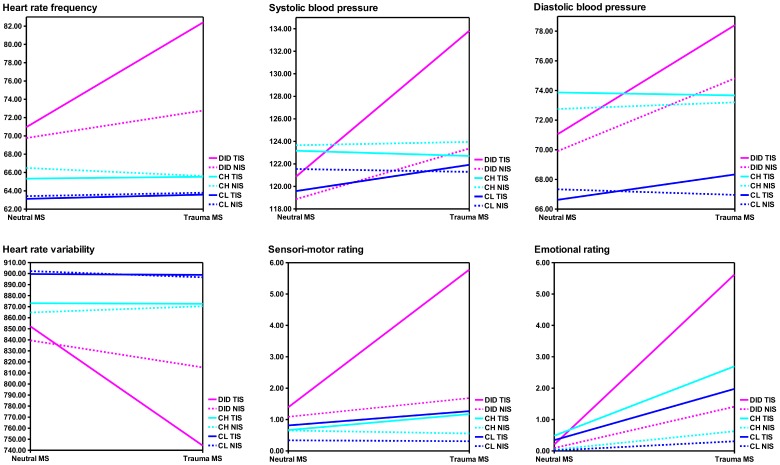
Methodology/principal findings: DID patients, high fantasy prone and low fantasy prone controls were studied in two different types of identity states (neutral and trauma-related) in an autobiographical memory script-driven (neutral or trauma-related) imagery paradigm. The controls were instructed to enact the two DID identity states. Twenty-nine subjects participated in the study: 11 patients with DID, 10 high fantasy prone DID simulating controls, and 8 low fantasy prone DID simulating controls. Autonomic and subjective reactions were obtained. Differences in psychophysiological and neural activation patterns were found between the DID patients and both high and low fantasy prone controls. That is, the identity states in DID were not convincingly enacted by DID simulating controls. Thus, important differences regarding regional cerebral bloodflow and psychophysiological responses for different types of identity states in patients with DID were upheld after controlling for DID simulation.
Conclusions/significance: The findings are at odds with the idea that differences among different types of dissociative identity states in DID can be explained by high fantasy proneness, motivated role-enactment, and suggestion. They indicate that DID does not have a sociocultural (e.g., iatrogenic) origin.
Conflict of interest statement
Figures





References
-
- Association AP, DSM-IV APATF on. Diagnostic and statistical manual of mental disorders: DSM-IV-TR. American Psychiatric Pub. 996 p. 2000.
-
- Piper A, Merskey H. The persistence of folly: a critical examination of dissociative identity disorder. Part I. The excesses of an improbable concept. Can J Psychiatry. 2004;49:592–600. - PubMed
-
- Piper A, Merskey H. The persistence of folly: critical examination of dissociative identity disorder. Part II. The defence and decline of multiple personality or dissociative identity disorder. Can J Psychiatry. 2004;49:678–683. - PubMed
-
- Coons PM. Re: the persistence of folly: a critical examination of dissociative identity disorder. Can J Psychiatry 50: 813; author reply 814. 2005. - PubMed
-
- Fraser GA. Re: the persistence of folly: a critical examination of dissociative identity disorder. Can J Psychiatry 50: 814; author reply 814. 2005. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
