

A prospective study of frailty in nephrology-referred patients with CKD
- PMID: 22770927
- PMCID: PMC3491110
- DOI: 10.1053/j.ajkd.2012.05.017
A prospective study of frailty in nephrology-referred patients with CKD
Abstract
Background: Frailty is a construct developed to characterize a state of reduced functional capacity in older adults. However, there are limited data describing the prevalence or consequences of frailty in middle-aged patients with chronic kidney disease (CKD).
Study design: Observational study.
Setting & participants: 336 non-dialysis-dependent patients with stages 1-4 CKD with estimated glomerular filtration rate (eGFR) <90 mL/min/1.73 m(2) (by the CKD-EPI [CKD Epidemiology Collaboration] serum creatinine-based equation) or evidence of microalbuminuria enrolled in the Seattle Kidney Study, a clinic-based cohort study. Findings were compared with community-dwelling older adults in the Cardiovascular Health Study.
Outcome: Prevalence and determinants of frailty in addition to its association with the combined outcome of all-cause mortality or renal replacement therapy.
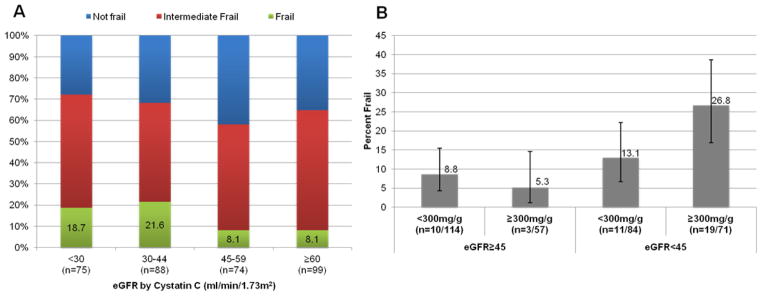
Measurements: We defined frailty according to established criteria as 3 or more of the following characteristics: slow gait, weakness, unintentional weight loss, exhaustion, and low physical activity. We estimated kidney function using serum cystatin C concentrations (eGFR(cys)) to minimize confounding due to relationships of serum creatinine levels with muscle mass and frailty.
Results: The mean age of the study population was 59 years and mean eGFR(cys) was 51 mL/min/1.73 m(2). The prevalence of frailty (14.0%) was twice that of the much older non-CKD reference population (P < 0.01). The most common frailty components were physical inactivity and exhaustion. After adjustment including diabetes, eGFR(cys) categories of <30 and 30-44 mL/min/1.73 m(2) were associated with a 2.8- (95% CI, 1.3-6.3) and 2.1 (95% CI, 1.0-4.7)-fold greater prevalence of frailty compared with GFR(cys) ≥60 mL/min/1.73 m(2). There were 63 events during a median 987 days of follow-up. After adjustment, the frailty phenotype was associated with an estimated 2.5 (95% CI, 1.4-4.4)-fold greater risk of death or dialysis therapy.
Limitations: Cross-sectional study design obscures inference regarding temporal relationships between CKD and frailty.
Conclusions: Frailty is relatively common in middle-aged patients with CKD and is associated with lower eGFR(cys) and increased risk of death or dialysis therapy.
Copyright © 2012 National Kidney Foundation, Inc. All rights reserved.
Figures


References
-
- Fried L, Tangen C, Walston J. Frailty in older adults: evidence for a phenotype. J of Gerontol. 2001;56A(3):M146–M156. - PubMed
-
- Cawthon P, Marshall L, Michael Y, et al. Frailty in older men: prevalence, progression, and relationship with mortality. Journal of the American Geriatrics Society. 2007;55(8):1216–1223. - PubMed
-
- Woods N, LaCroix A, Gray S, et al. Frailty: emergence and consequences in women aged 65 and older in the Women’s Health Initiative Observational Study. Journal of the American Geriatrics Society. 2005;53(8):1321–1330. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
