

Challenges in the diagnosis & treatment of miliary tuberculosis
- PMID: 22771605
- PMCID: PMC3401706
Challenges in the diagnosis & treatment of miliary tuberculosis
Abstract
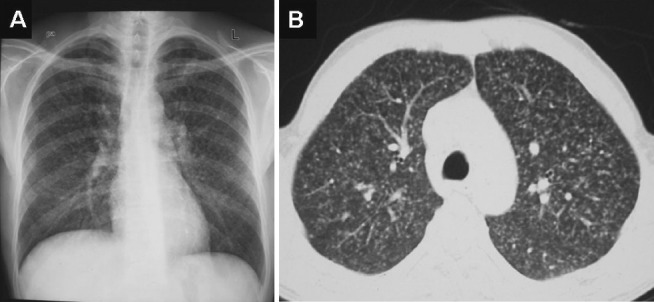
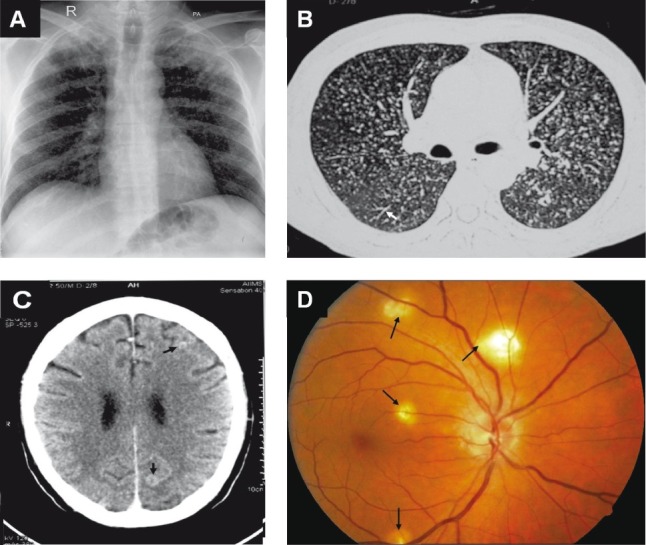
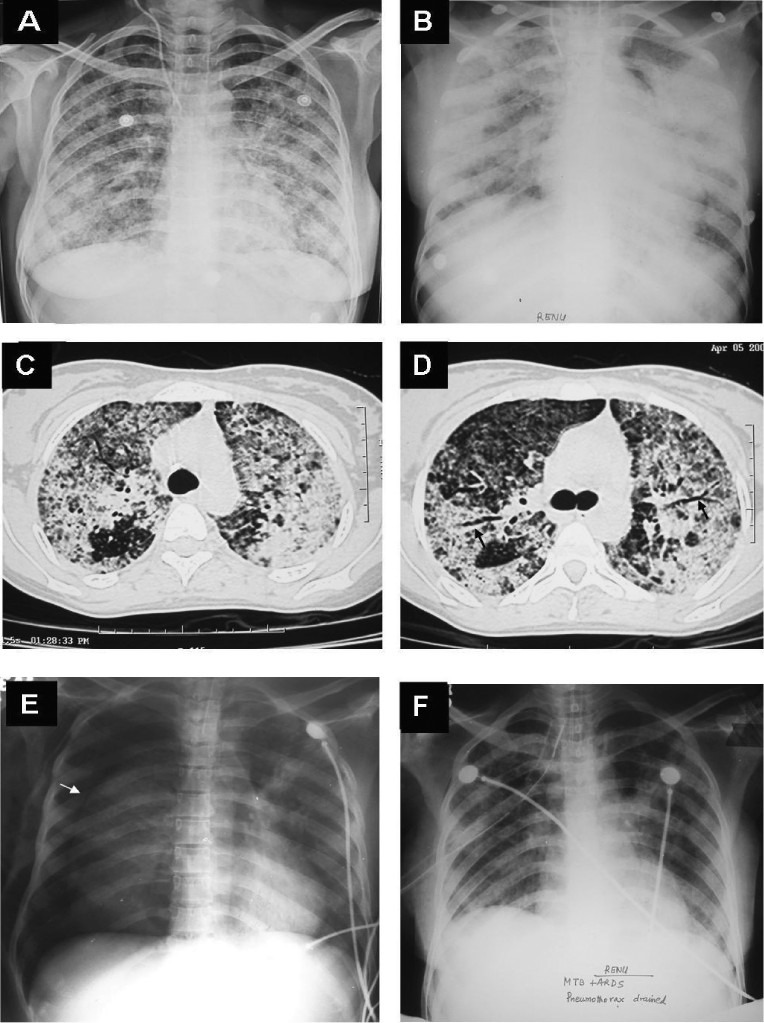
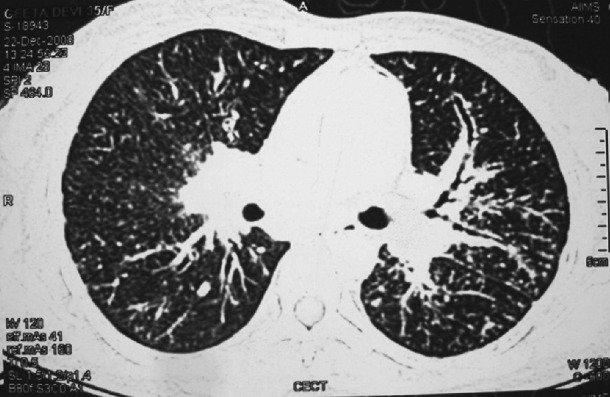
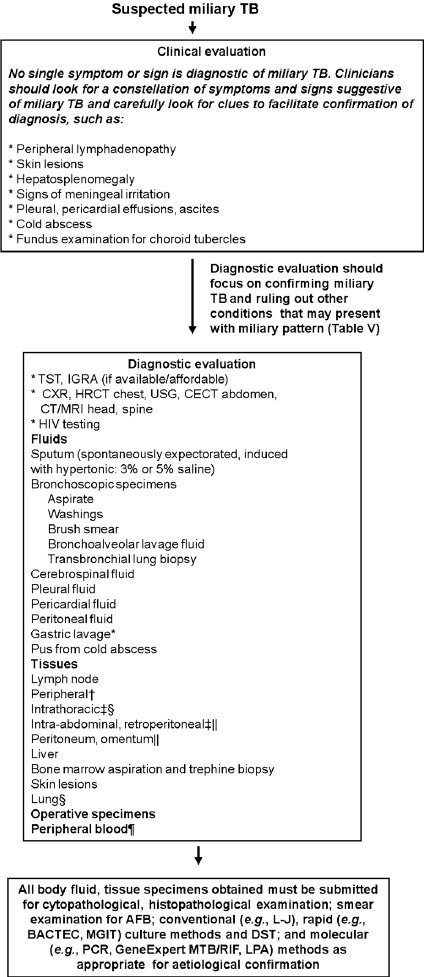
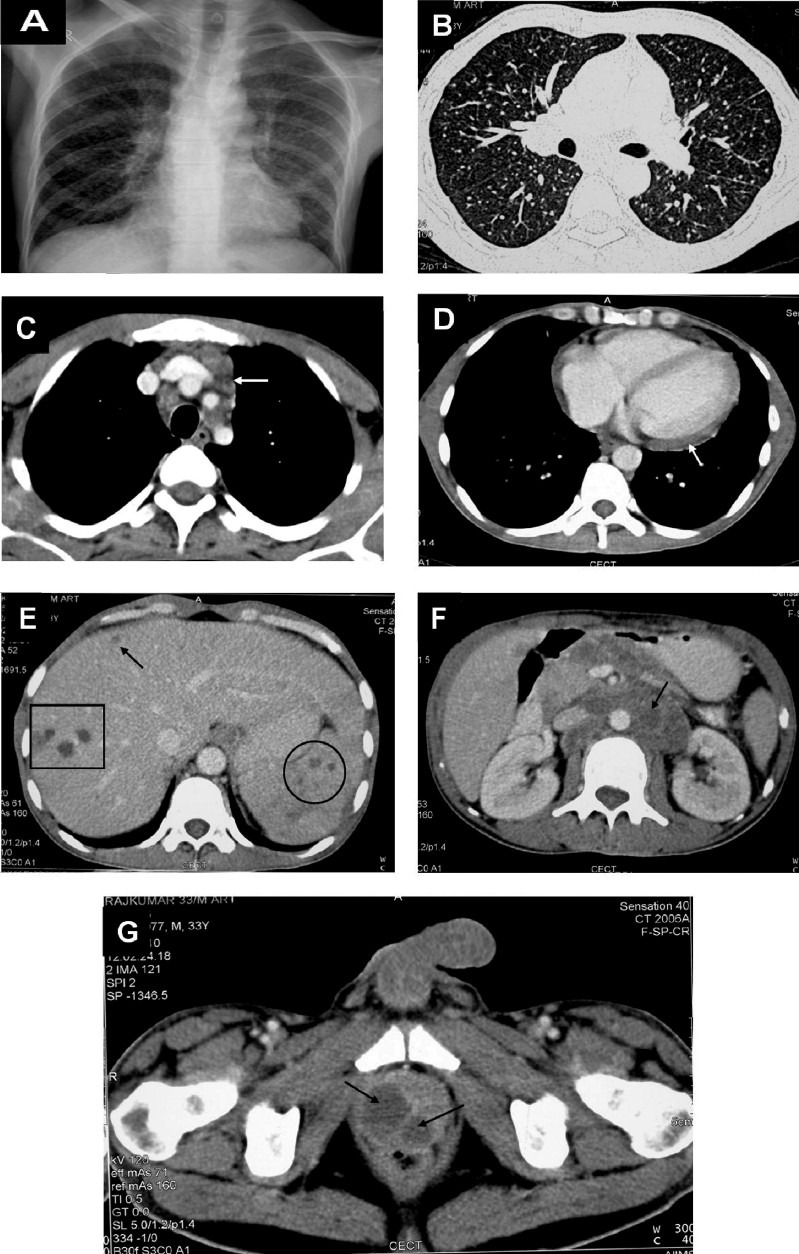
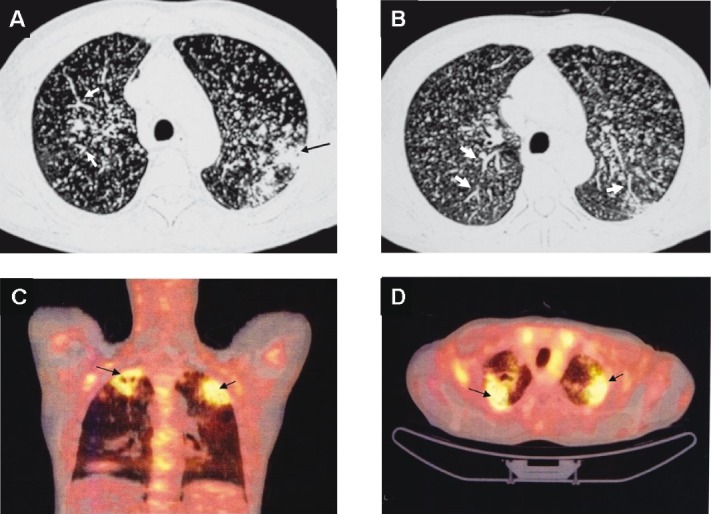
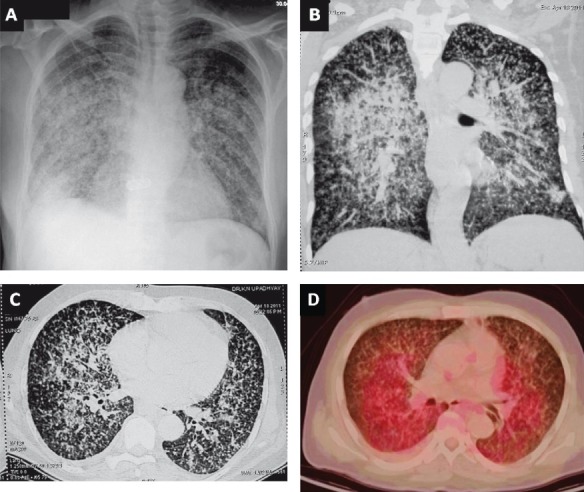
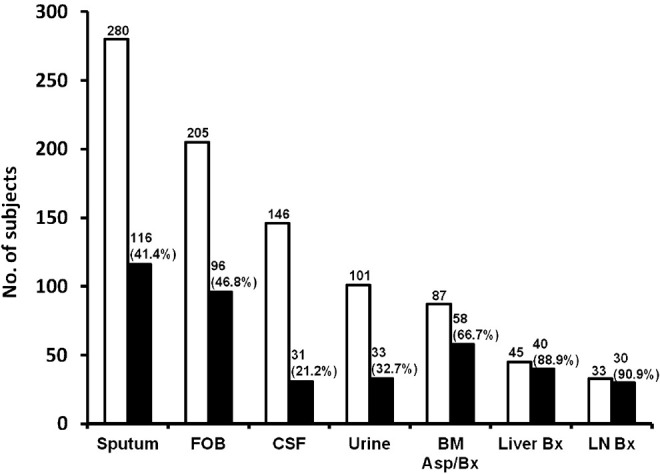
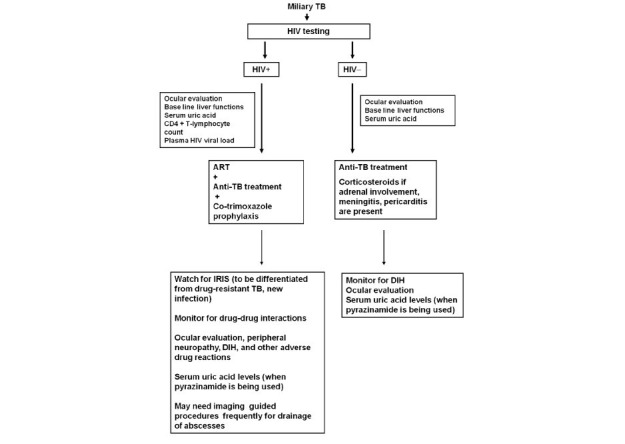
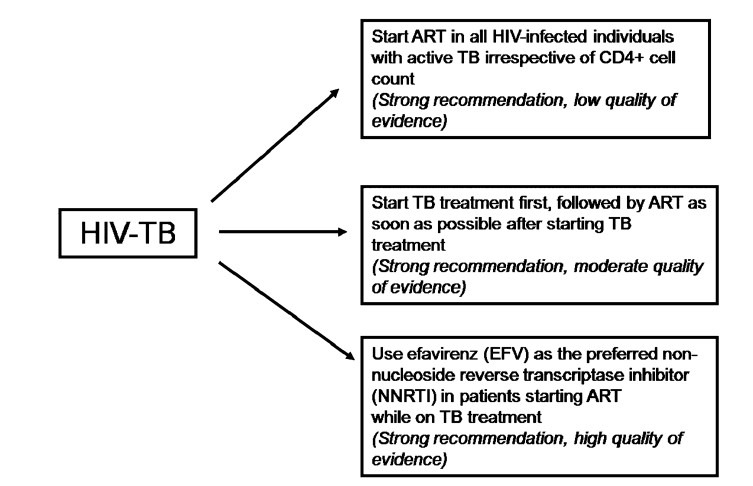
Miliary tuberculosis (TB) is a potentially lethal disease if not diagnosed and treated early. Diagnosing miliary TB can be a challenge that can perplex even the most experienced clinicians. Clinical manifestations are nonspecific, typical chest radiograph findings may not be evident till late in the disease, high resolution computed tomography (HRCT) shows randomly distributed miliary nodules and is relatively more sensitive. Ultrasonography, CT and magnetic resonance imaging (MRI) are useful in discerning the extent of organ involvement by lesions of miliary TB in extra-pulmonary locations. Fundus examination for choroid tubercles, histopathological examination of tissue biopsy specimens, conventional and rapid culture methods for isolation of Mycobacterium tuberculosis, drug-susceptibility testing, along with use of molecular biology tools in sputum, body fluids, other body tissues are useful in confirming the diagnosis. Although several prognostic markers have been described which predict mortality, yet untreated miliary TB has a fatal outcome within one year. A high index of clinical suspicion and early diagnosis and timely institution of anti-tuberculosis treatment can be life-saving. Response to first-line anti-tuberculosis drugs is good but drug-induced hepatotoxicity and drug-drug interactions in human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) patients pose significant problems during treatment. However, sparse data are available from randomized controlled trials to define the optimum regimen and duration of treatment in patients with drug-sensitive as well as drug-resistant miliary TB, including those with HIV/AIDS.
Figures


References
-
- Manget JJ. Sepulchretum sive anatomica practica. Vol. 1. London: Cramer and Perachon; 1700. Observatio XLVII (3 vols)
-
- Sahn SA, Neff TA. Miliary tuberculosis. Am J Med. 1974;56:494–505. - PubMed
-
- Sharma SK, Mohan A. Miliary tuberculosis. In: Schlossberg D, editor. Tuberculosis and nontuberculous mycobacterial infections. 6th ed. Washington: American Society for Microbiology Press; 2011. pp. 415–35.
-
- Sharma SK, Mohan A, Sharma A, Mitra DK. Miliary tuberculosis: new insights into an old disease. Lancet Infect Dis. 2005;5:415–30. - PubMed
-
- Alvarez S, McCabe WR. Extrapulmonary tuberculosis revisited: a review of experience at Boston City and other hospitals. Medicine (Baltimore) 1984;63:25–55. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources