

Inflammatory and injury signals released from the post-stenotic human kidney
- PMID: 22771675
- PMCID: PMC3572435
- DOI: 10.1093/eurheartj/ehs197
Inflammatory and injury signals released from the post-stenotic human kidney
Abstract
Aims: The mechanisms mediating kidney injury and repair in humans with atherosclerotic renal artery stenosis (ARAS) remain poorly understood. We hypothesized that the stenotic kidney releases inflammatory mediators and recruits progenitor cells to promote regeneration.
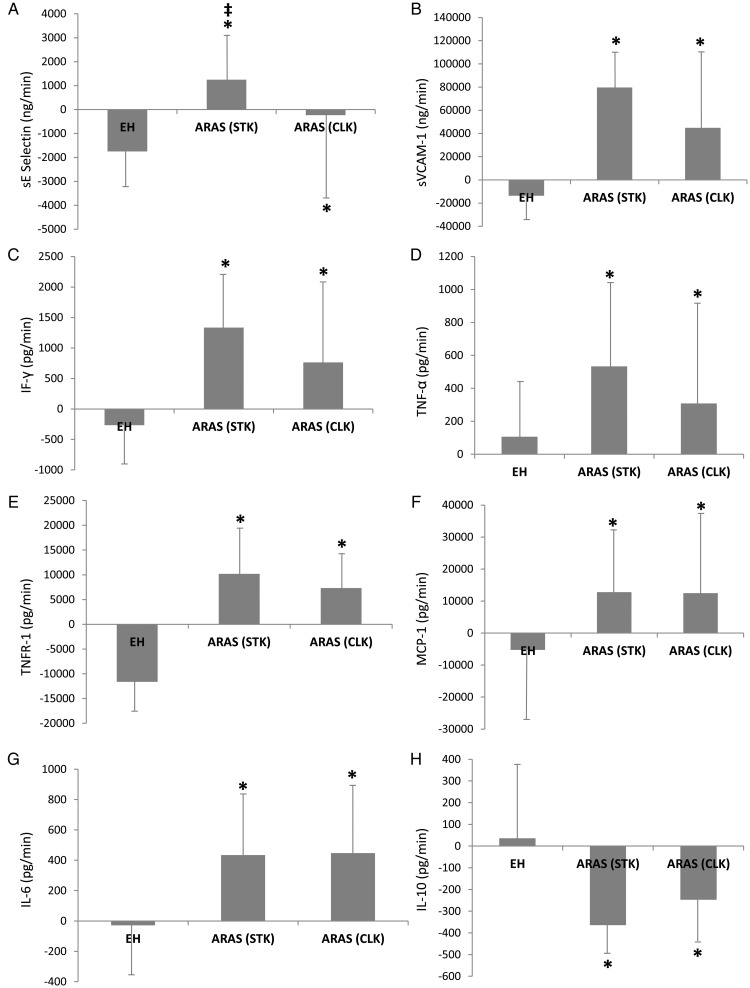
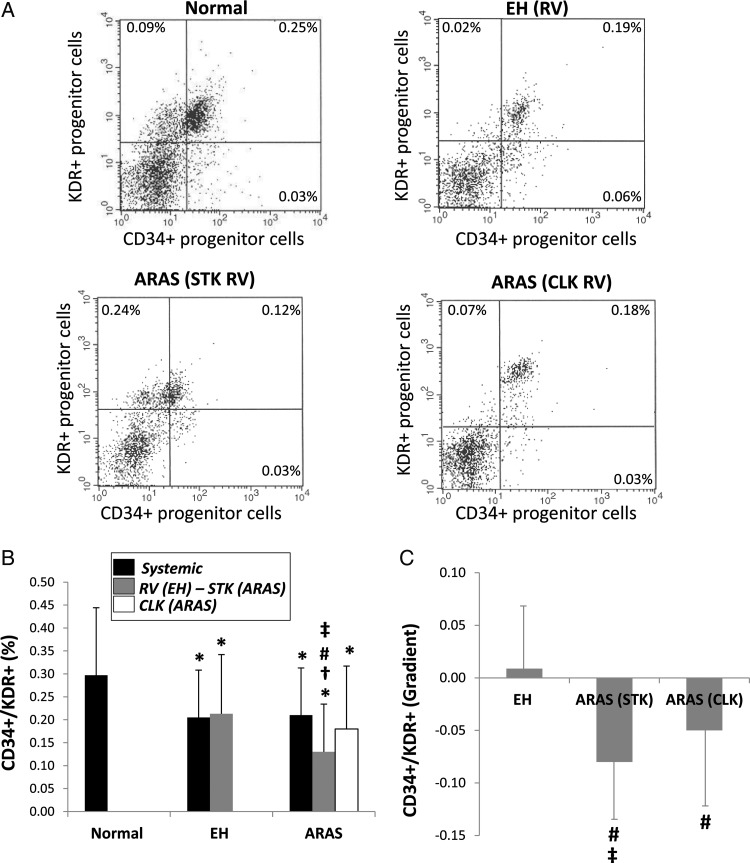
Methods and results: Essential hypertensive (EH) and ARAS patients (n=24 each) were studied during controlled sodium intake and antihypertensive treatment. Inferior vena cava (IVC) and renal vein (RV) levels of CD34+/KDR+ progenitor cells, cell adhesion molecules, inflammatory biomarkers, progenitor cell homing signals, and pro-angiogenic factors were measured in EH and ARAS, and their gradient and net release compared with systemic levels in matched normotensive controls (n= 24). Blood pressure in ARAS was similar to EH, but the glomerular filtration rate was lower. Renal vein levels of soluble E-Selectin, vascular cell adhesion molecule-1, and several inflammatory markers were higher in the stenotic kidney RV vs. normal and EH RV (P < 0.05), and their net release increased. Similarly, stem-cell homing factor levels increased in the stenotic kidney RV. Systemic CD34+/KDR+ progenitor cell levels were lower in both EH and ARAS and correlated with cytokine levels. Moreover, CD34+/KDR+ progenitor cells developed a negative gradient across the ARAS kidney, suggesting progenitor cell retention. The non-stenotic kidney also showed signs of inflammatory processes, which were more subtle than in the stenotic kidney.
Conclusion: Renal vein blood from post-stenotic human kidneys has multiple markers reflecting active inflammation that portends kidney injury and reduced function. CD34+/KDR+ progenitor cells sequestered within these kidneys may participate in reparative processes. These inflammation-related pathways and limited circulating progenitor cells may serve as novel therapeutic targets to repair the stenotic kidney.
Figures
References
-
- Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jr, Jones DW, Materson BJ, Oparil S, Wright JT, Jr, Roccella EJ. Seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension. 2003;42:1206–1252. - PubMed
-
- Hansen KJ, Edwards MS, Craven TE, Cherr GS, Jackson SA, Appel RG, Burke GL, Dean RH. Prevalence of renovascular disease in the elderly: a population-based study. J Vasc Surg. 2002;36:443–451. - PubMed
-
- Kalra PA, Guo H, Kausz AT, Gilbertson DT, Liu J, Chen SC, Ishani A, Collins AJ, Foley RN. Atherosclerotic renovascular disease in united states patients aged 67 years or older: risk factors, revascularization, and prognosis. Kidney Int. 2005;68:293–301. - PubMed
-
- Losito A, Fagugli RM, Zampi I, Parente B, de Rango P, Giordano G, Cao P. Comparison of target organ damage in renovascular and essential hypertension. Am J Hypertens. 1996;9:1062–1067. - PubMed
-
- Minuz P, Patrignani P, Gaino S, Degan M, Menapace L, Tommasoli R, Seta F, Capone ML, Tacconelli S, Palatresi S, Bencini C, Del Vecchio C, Mansueto G, Arosio E, Santonastaso CL, Lechi A, Morganti A, Patrono C. Increased oxidative stress and platelet activation in patients with hypertension and renovascular disease. Circulation. 2002;106:2800–2805. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
