

Development and evaluation of an interprofessional communication intervention to improve family outcomes in the ICU
- PMID: 22772089
- PMCID: PMC3823241
- DOI: 10.1016/j.cct.2012.06.010
Development and evaluation of an interprofessional communication intervention to improve family outcomes in the ICU
Abstract
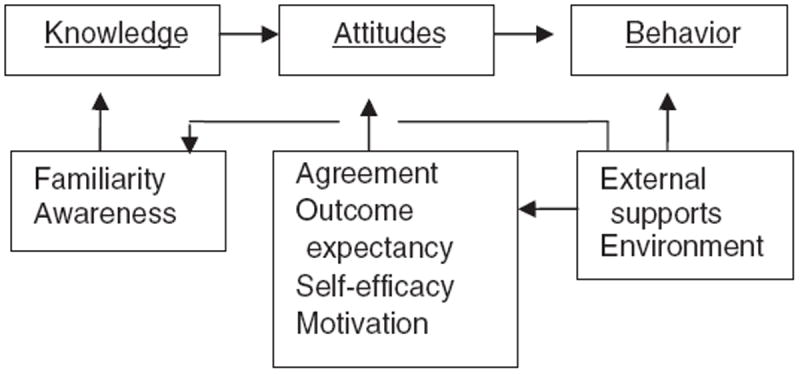
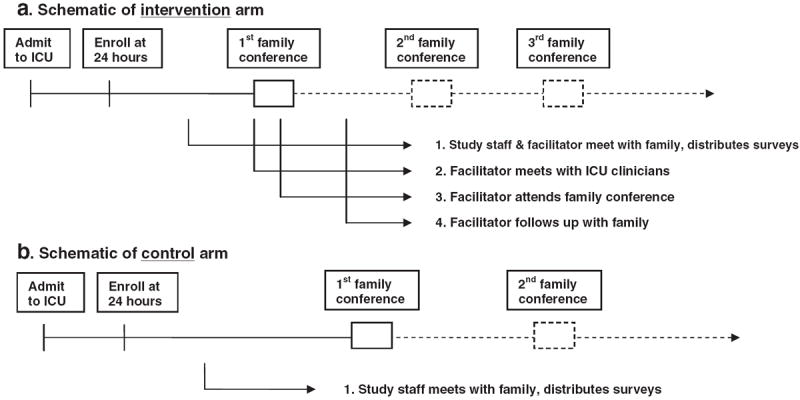
The intensive care unit (ICU), where death is common and even survivors of an ICU stay face the risk of long-term morbidity and re-admissions to the ICU, represents an important setting for improving communication about palliative and end-of-life care. Communication about the goals of care in this setting should be a high priority since studies suggest that the current quality of ICU communication is often poor and is associated with psychological distress among family members of critically ill patients. This paper describes the development and evaluation of an intervention designed to improve the quality of care in the ICU by improving communication among the ICU team and with family members of critically ill patients. We developed a multi-faceted, interprofessional intervention based on self-efficacy theory. The intervention involves a "communication facilitator" - a nurse or social worker - trained to facilitate communication among the interprofessional ICU team and with the critically ill patient's family. The facilitators are trained using three specific content areas: a) evidence-based approaches to improving clinician-family communication in the ICU, b) attachment theory allowing clinicians to adapt communication to meet individual family member's communication needs, and c) mediation to facilitate identification and resolution of conflict including clinician-family, clinician-clinician, and intra-family conflict. The outcomes assessed in this randomized trial focus on psychological distress among family members including anxiety, depression, and post-traumatic stress disorder at 3 and 6 months after the ICU stay. This manuscript also reports some of the lessons that we have learned early in this study.
Trial registration: ClinicalTrials.gov NCT00720200.
Copyright © 2012 Elsevier Inc. All rights reserved.
Figures
References
-
- Angus DC, Barnato AE, Linde-Zwirble WT, et al. Use of intensive care at the end of life in the United States: an epidemiologic study. Crit Care Med. 2004;32:638–43. - PubMed
-
- Heyland DK, Hopman W, Coo H, Tranmar J, McColl MA. Long-term health-related quality of life in survivors of sepsis. Crit Care Med. 2000;28:3599–605. - PubMed
-
- Curtis JR, Vincent JL. Ethics and end-of-life care for adults in the intensive care unit. Lancet. 2010;376:1347–53. - PubMed
-
- Caswell D, Omrey A. The dying patient in the intensive care unit: making the critical difference. Clin Issues Crit Care Nurs. 1990;1:178–86. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
